Wasan Ajay D, Jamison Robert N, Pham Loc, Tipirneni Naveen, Nedeljkovic Srdjan S, Katz Jeffrey N
Department of Anesthesiology, Brigham & Women's Hospital and Harvard Medical School, Boston, MA, USA.
BMC Musculoskelet Disord. 2009 Feb 16;10:22. doi: 10.1186/1471-2474-10-22.
Comorbid psychopathology is an important predictor of poor outcome for many types of treatments for back or neck pain. But it is unknown if this applies to the results of medial branch blocks (MBBs) for chronic low back or neck pain, which involves injecting the medial branch of the dorsal ramus nerves that innervate the facet joints. The objective of this study was to determine whether high levels of psychopathology are predictive of pain relief after MBB injections in the lumbar or cervical spine.
This was a prospective cohort study. Consecutive patients in a pain medicine practice undergoing MBBs of the lumbar or cervical facets with corticosteroids were recruited to participate. Subjects were selected for a MBB based on operationalized selection criteria and the procedure was performed in a standardized manner. Subjects completed the Brief Pain Inventory (BPI) and the Hospital Anxiety and Depression Scale (HADS) just prior to the procedure and at one-month follow up. Scores on the HADS classified the subjects into three groups based on psychiatric symptoms, which formed the primary predictor variable: Low, Moderate, or High levels of psychopathology. The primary outcome measure was the percent improvement in average daily pain rating one-month following an injection. Analysis of variance and chi-square were used to analyze the analgesia and functional rating differences between groups, and to perform a responder analysis.
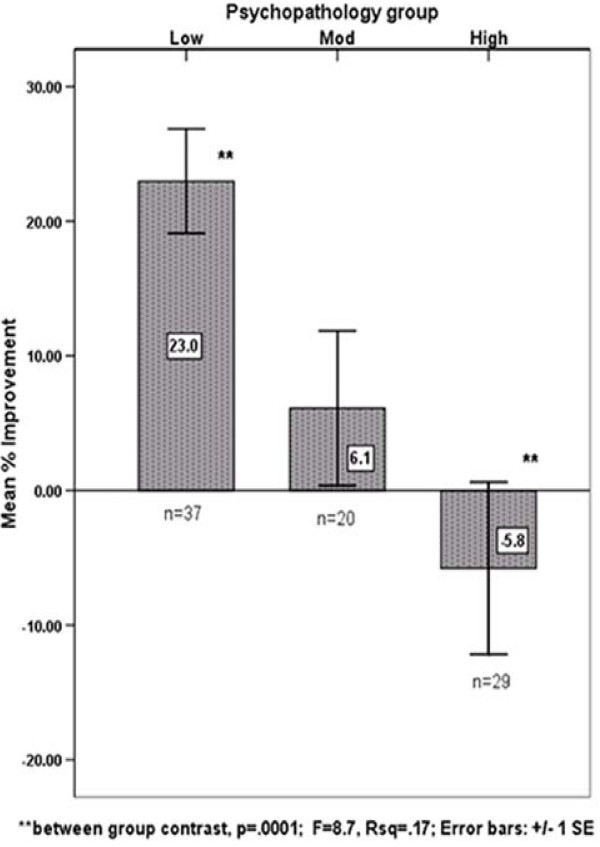
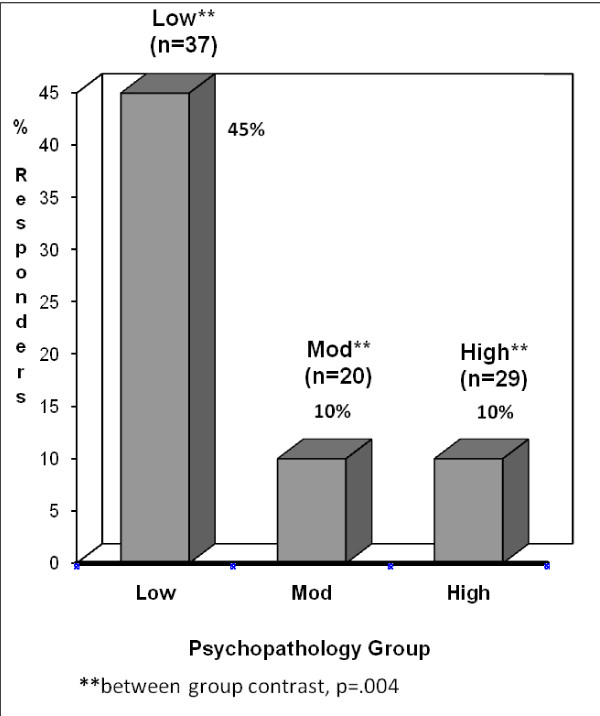
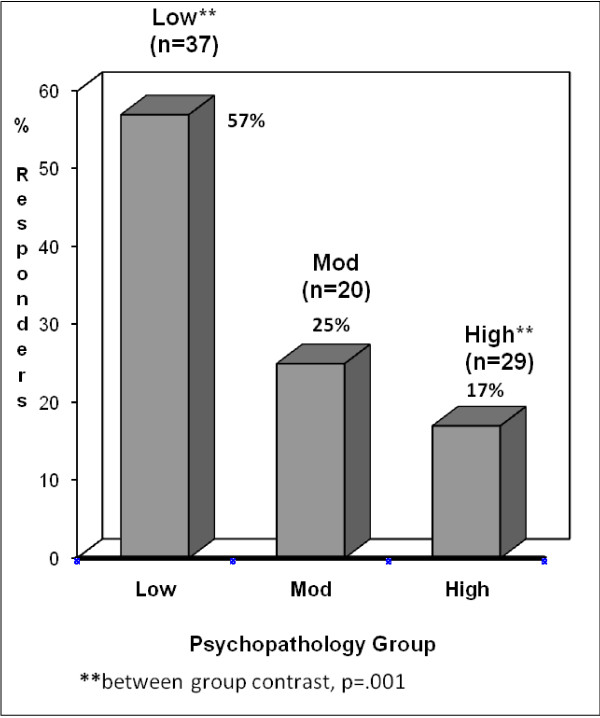
Eighty six (86) subjects completed the study. The Low psychopathology group (n = 37) reported a mean of 23% improvement in pain at one-month while the High psychopathology group (n = 29) reported a mean worsening of -5.8% in pain (p < .001). Forty five percent (45%) of the Low group had at least 30% improvement in pain versus 10% in the High group (p < .001). Using an analysis of covariance, no baseline demographic, social, or medical variables were significant predictors of pain improvement, nor did they mitigate the effect of psychopathology on the outcome.
Psychiatric comorbidity is associated with diminished pain relief after a MBB injection performed with steroid at one-month follow-up. These findings illustrate the importance of assessing comorbid psychopathology as part of a spine care evaluation.
共病精神病理学是许多类型的背部或颈部疼痛治疗效果不佳的重要预测因素。但尚不清楚这是否适用于慢性下背部或颈部疼痛的内侧支阻滞(MBB)结果,该阻滞涉及注射支配小关节的背侧支神经的内侧支。本研究的目的是确定高水平的精神病理学是否可预测腰椎或颈椎MBB注射后的疼痛缓解情况。
这是一项前瞻性队列研究。招募了在疼痛医学实践中连续接受腰椎或颈椎小关节皮质类固醇MBB治疗的患者参与。根据实施的选择标准选择接受MBB治疗的受试者,并以标准化方式进行该操作。受试者在操作前和随访1个月时完成简短疼痛问卷(BPI)和医院焦虑抑郁量表(HADS)。根据精神症状,HADS评分将受试者分为三组,形成主要预测变量:低、中或高水平的精神病理学。主要结局指标是注射后1个月平均每日疼痛评分的改善百分比。采用方差分析和卡方检验分析组间镇痛和功能评分差异,并进行反应者分析。
86名受试者完成了研究。低精神病理学组(n = 37)报告1个月时疼痛平均改善23%,而高精神病理学组(n = 29)报告疼痛平均恶化-5.8%(p <.001)。低组45%的患者疼痛至少改善30%,而高组为10%(p <.001)。使用协方差分析,没有基线人口统计学、社会或医学变量是疼痛改善的显著预测因素,它们也没有减轻精神病理学对结局的影响。
在随访1个月时,共病精神疾病与类固醇注射的MBB后疼痛缓解减少有关。这些发现说明了评估共病精神病理学作为脊柱护理评估一部分的重要性。