Mwai Leah, Ochong Edwin, Abdirahman Abdi, Kiara Steven M, Ward Steve, Kokwaro Gilbert, Sasi Philip, Marsh Kevin, Borrmann Steffen, Mackinnon Margaret, Nzila Alexis
Kenya Medical Research Institute/Wellcome Trust Collaborative Research Programme, Kilifi, Kenya.
Malar J. 2009 May 18;8:106. doi: 10.1186/1475-2875-8-106.
The spread of resistance to chloroquine (CQ) led to its withdrawal from use in most countries in sub-Saharan Africa in the 1990s. In Malawi, this withdrawal was followed by a rapid reduction in the frequency of resistance to the point where the drug is now considered to be effective once again, just nine years after its withdrawal. In this report, the polymorphisms of markers associated with CQ-resistance against Plasmodium falciparum isolates from coastal Kenya (Kilifi) were investigated, from 1993, prior to the withdrawal of CQ, to 2006, seven years after its withdrawal. Changes to those that occurred in the dihydrofolate reductase gene (dhfr) that confers resistance to the replacement drug, pyrimethamine/sulphadoxine were also compared.
Mutations associated with CQ resistance, at codons 76 of pfcrt, at 86 of pfmdr1, and at codons 51, 59 and 164 of dhfr were analysed using PCR-restriction enzyme methods. In total, 406, 240 and 323 isolates were genotyped for pfcrt-76, pfmdr1-86 and dhfr, respectively.
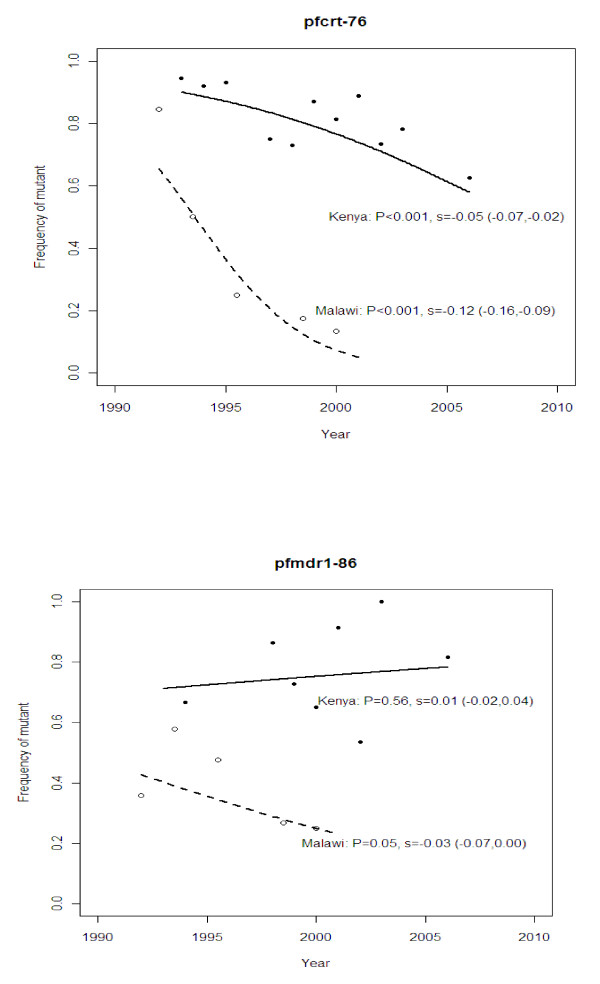
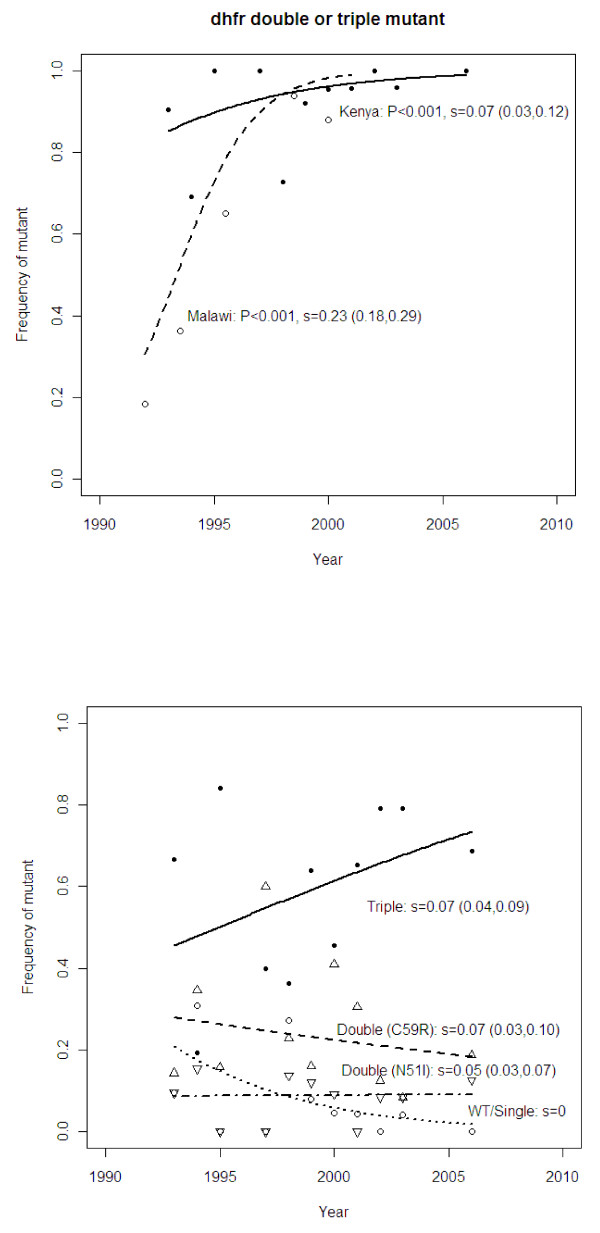
From 1993 to 2006, the frequency of the pfcrt-76 mutant significantly decreased from around 95% to 60%, while the frequency of pfmdr1-86 did not decline, remaining around 75%. Though the frequency of dhfr mutants was already high (around 80%) at the start of the study, this frequency increased to above 95% during the study period. Mutation at codon 164 of dhfr was analysed in 2006 samples, and none of them had this mutation.
In accord with the study in Malawi, a reduction in resistance to CQ following official withdrawal in 1999 was found, but unlike Malawi, the decline of resistance to CQ in Kilifi was much slower. It is estimated that, at current rates of decline, it will take 13 more years for the clinical efficacy of CQ to be restored in Kilifi. In addition, CQ resistance was declining before the drug's official withdrawal, suggesting that, prior to the official ban, the use of CQ had decreased, probably due to its poor clinical effectiveness.
对氯喹(CQ)耐药性的传播导致其在20世纪90年代在撒哈拉以南非洲的大多数国家停止使用。在马拉维,这种停用之后耐药频率迅速下降,直至现在,在停用仅仅九年后,该药物再次被认为是有效的。在本报告中,对1993年(CQ停用之前)至2006年(CQ停用七年之后)肯尼亚沿海地区(基利菲)恶性疟原虫分离株中与CQ耐药性相关标志物的多态性进行了研究。还比较了对替代药物乙胺嘧啶/磺胺多辛产生耐药性的二氢叶酸还原酶基因(dhfr)中发生的变化。
使用PCR-限制性酶切方法分析与CQ耐药性相关的突变,这些突变分别位于pfcrt的第76位密码子、pfmdr1的第86位密码子以及dhfr的第51、59和164位密码子。总共分别对406、240和323株分离株进行了pfcrt-76、pfmdr1-86和dhfr的基因分型。
从1993年到2006年,pfcrt-76突变体的频率从约95%显著下降至60%,而pfmdr1-86的频率没有下降,仍保持在75%左右。尽管在研究开始时dhfr突变体的频率已经很高(约80%),但在研究期间该频率增加到了95%以上。在2006年的样本中分析了dhfr第164位密码子的突变,没有一个样本有此突变。
与马拉维的研究一致,发现1999年官方停用CQ后对其耐药性有所降低,但与马拉维不同的是,基利菲对CQ耐药性的下降要慢得多。据估计,按照目前的下降速度,基利菲恢复CQ临床疗效还需要13年时间。此外,在药物正式停用之前CQ耐药性就在下降,这表明在官方禁令之前,CQ的使用可能因临床效果不佳而减少。