Department of National Defence, Canadian Forces, Mount Sinai Hospital Toronto/University Health Network, University of Toronto, 600 University Avenue, Toronto, ON, Canada.
Crit Care. 2009;13(5):R170. doi: 10.1186/cc8146. Epub 2009 Oct 29.
The objective of this pilot study was to assess the usability of the draft Ontario triage protocol, to estimate its potential impact on patient outcomes, and ability to increase resource availability based on a retrospective cohort of critically ill patients cared for during a non-pandemic period.
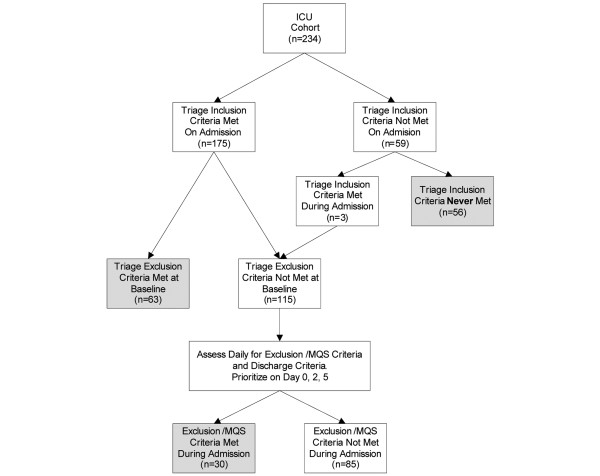
Triage officers applied the protocol prospectively to 2 retrospective cohorts of patients admitted to 2 academic medical/surgical ICUs during an 8 week period of peak occupancy. Each patient was assigned a treatment priority (red -- 'highest', yellow -- 'intermediate', green -- 'discharge to ward', or blue/black -- 'expectant') by the triage officers at 3 separate time points (at the time of admission to the ICU, 48, and 120 hours post admission).
Overall, triage officers were either confident or very confident in 68.4% of their scores; arbitration was required in 54.9% of cases. Application of the triage protocol would potentially decrease the number of required ventilator days by 49.3% (568 days) and decrease the total ICU days by 52.6% (895 days). On the triage protocol at ICU admission the survival rate in the red (93.7%) and yellow (62.5%) categories were significantly higher then that of the blue category (24.6%) with associated P values of < 0.0001 and 0.0003 respectively. Further, the survival rate of the red group was significantly higher than the overall survival rate of 70.9% observed in the cohort (P < 0.0001). At 48 and 120 hours, survival rates in the blue group increased but remained lower then the red or yellow groups.
Refinement of the triage protocol and implementation is required prior to future study, including improved training of triage officers, and protocol modification to minimize the exclusion from critical care of patients who may in fact benefit. However, our results suggest that the triage protocol can help to direct resources to patients who are most likely to benefit, and help to decrease the demands on critical care resources, thereby making available more resources to treat other critically ill patients.
本研究旨在评估安大略省分诊协议草案的可用性,估算其对患者结局的潜在影响,并评估该协议能否基于非大流行时期入住 2 家学术性医疗/外科重症监护病房(ICU)的重症患者的回顾性队列,增加资源的可用性。
分诊员前瞻性地将该协议应用于 2 个队列,每个队列均包括在入住高峰期的 8 周内入住 2 家学术性医疗/外科 ICU 的患者。每个患者均由分诊员在 3 个不同时间点(入住 ICU 时、48 小时和 120 小时后)根据协议被分配治疗优先级(红色——“最高”,黄色——“中等”,绿色——“转至病房”,或蓝色/黑色——“期待”)。
总体而言,分诊员对其评分的信心程度为 68.4%;在 54.9%的病例中需要仲裁。应用分诊协议可将所需呼吸机天数减少 49.3%(568 天),将 ICU 总天数减少 52.6%(895 天)。在 ICU 入住时的分诊协议中,红色(93.7%)和黄色(62.5%)类别的生存率明显高于蓝色类别(24.6%),相应的 P 值分别为<0.0001 和 0.0003。此外,红色组的生存率明显高于队列中观察到的总体生存率 70.9%(P<0.0001)。在 48 小时和 120 小时,蓝色组的生存率增加,但仍低于红色或黄色组。
在未来的研究之前,需要对分诊协议进行细化和实施,包括分诊员的强化培训,以及协议的修改,以尽量减少将可能受益的患者排除在重症监护之外。然而,我们的结果表明,分诊协议可以帮助将资源导向最有可能受益的患者,并有助于减少对重症监护资源的需求,从而为治疗其他重症患者提供更多资源。