SUNY at Albany, School of Public Health, Rensselaer NY, USA.
BMC Infect Dis. 2009 Dec 14;9:203. doi: 10.1186/1471-2334-9-203.
The risk and course of serum transaminase elevations (TEs) and clinical hepatic serious adverse event (SAE) development in ritonavir-boosted tipranavir (TPV/r) 500/200 mg BID recipients, who also received additional combination antiretroviral treatment agents in clinical trials (TPV/r-based cART), was determined.
Aggregated transaminase and hepatic SAE data through 96 weeks of TPV/r-based cART from five Phase IIb/III trials were analyzed. Patients were categorized by the presence or absence of underlying liver disease (+LD or -LD). Kaplan-Meier (K-M) probability estimates for time-to-first US National Institutes of Health, Division of AIDS (DAIDS) Grade 3/4 TE and clinical hepatic SAE were determined and clinical actions/outcomes evaluated. Risk factors for DAIDS Grade 3/4 TE were identified through multivariate Cox regression statistical modeling.
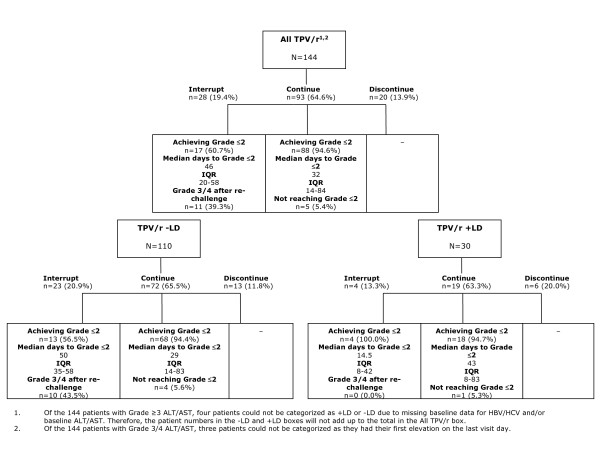
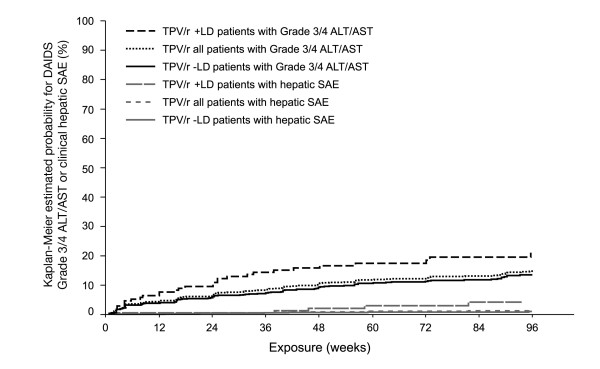
Grade 3/4 TEs occurred in 144/1299 (11.1%) patients; 123/144 (85%) of these were asymptomatic; 84% of these patients only temporarily interrupted treatment or continued, with transaminase levels returning to Grade < or = 2. At 96 weeks of study treatment, the incidence of Grade 3/4 TEs was higher among the +LD (16.8%) than among the -LD (10.1%) patients. K-M analysis revealed an incremental risk for developing DAIDS Grade 3/4 TEs; risk was greatest through 24 weeks (6.1%), and decreasing thereafter (>24-48 weeks: 3.4%, >48 weeks-72 weeks: 2.0%, >72-96 weeks: 2.2%), and higher in +LD than -LD patients at each 24-week interval. Treatment with TPV/r, co-infection with hepatitis B and/or C, DAIDS grade >1 TE and CD4+ > 200 cells/mm3 at baseline were found to be independent risk factors for development of DAIDS Grade 3/4 TE; the hazard ratios (HR) were 2.8, 2.0, 2.1 and 1.5, respectively. Four of the 144 (2.7%) patients with Grade 3/4 TEs developed hepatic SAEs; overall, 14/1299 (1.1%) patients had hepatic SAEs including six with hepatic failure (0.5%). The K-M risk of developing hepatic SAEs through 96 weeks was 1.4%; highest risk was observed during the first 24 weeks and decreased thereafter; the risk was similar between +LD and -LD patients for the first 24 weeks (0.6% and 0.5%, respectively) and was higher for +LD patients, thereafter.
Through 96 weeks of TPV/r-based cART, DAIDS Grade 3/4 TEs and hepatic SAEs occurred in approximately 11% and 1% of TPV/r patients, respectively; most (84%) had no significant clinical implications and were managed without permanent treatment discontinuation. Among the 14 patients with hepatic SAE, 6 experienced hepatic failure (0.5%); these patients had profound immunosuppression and the rate appears higher among hepatitis co-infected patients. The overall probability of experiencing a hepatic SAE in this patient cohort was 1.4% through 96 weeks of treatment. Independent risk factors for DAIDS Grade 3/4 TEs include TPV/r treatment, co-infection with hepatitis B and/or C, DAIDS grade >1 TE and CD4+ > 200 cells/mm3 at baseline.
US-NIH Trial registration number: NCT00144170.
在接受利托那韦增强的替拉那韦(TPV/r)500/200 毫克,每日两次联合其他抗逆转录病毒治疗药物的临床试验(TPV/r 为基础的 cART)的患者中,确定了血清转氨酶升高(TEs)和临床严重肝不良事件(SAE)发展的风险和过程。
分析了来自五个 IIb/III 期临床试验的 96 周 TPV/r 为基础的 cART 的汇总转氨酶和肝 SAE 数据。根据是否存在基础肝病(+LD 或-LD)对患者进行分类。确定首次出现美国国立卫生研究院(NIH)、艾滋病司(DAIDS)3/4 级 TE 和临床肝 SAE 的时间的 Kaplan-Meier(K-M)概率估计值,并评估临床操作/结果。通过多变量 Cox 回归统计模型确定 DAIDS 3/4 级 TE 的危险因素。
144/1299(11.1%)例患者发生 3/4 级 TEs;其中 123/144(85%)例无症状;这些患者中有 84%仅暂时中断治疗或继续治疗,转氨酶水平恢复至<或=2 级。在研究治疗的第 96 周,+LD(16.8%)患者发生 3/4 级 TEs 的发生率高于-LD(10.1%)患者。K-M 分析显示发生 DAIDS 3/4 级 TEs 的风险增加;风险在 24 周时最大(6.1%),此后逐渐降低(>24-48 周:3.4%,>48-72 周:2.0%,>72-96 周:2.2%),在每个 24 周间隔,+LD 患者的风险均高于-LD 患者。TPV/r 治疗、乙型肝炎和/或丙型肝炎合并感染、DAIDS 分级>1 TE 和基线时 CD4+>200 个细胞/mm3 被发现是发生 DAIDS 3/4 级 TE 的独立危险因素;危险比(HR)分别为 2.8、2.0、2.1 和 1.5。144 例 3/4 级 TE 患者中有 4 例(2.7%)发展为肝 SAE;总的来说,1299 例患者中有 14 例(1.1%)发生肝 SAE,包括 6 例肝衰竭(0.5%)。在 96 周内发生肝 SAE 的 K-M 风险为 1.4%;风险在最初 24 周最高,此后逐渐降低;在最初 24 周,+LD 和-LD 患者的风险相似(分别为 0.6%和 0.5%),此后,+LD 患者的风险更高。
在接受 TPV/r 为基础的 cART 的 96 周内,TPV/r 患者分别有 11%和 1%发生 DAIDS 3/4 级 TEs 和肝 SAE;大多数(84%)没有明显的临床意义,不需要永久性停药。在 14 例肝 SAE 患者中,有 6 例发生肝衰竭(0.5%);这些患者存在严重的免疫抑制,乙型肝炎合并感染患者的发生率似乎更高。在该患者队列中,通过 96 周的治疗,总体发生肝 SAE 的概率为 1.4%。DAIDS 3/4 级 TE 的独立危险因素包括 TPV/r 治疗、乙型肝炎和/或丙型肝炎合并感染、DAIDS 分级>1 TE 和基线时 CD4+>200 个细胞/mm3。
美国国立卫生研究院(NIH)试验注册号:NCT00144170。