Hartel Mark, Illing Peter, Mercer James B, Lademann Jürgen, Daeschlein Georg, Hoffmann Gerd
Technical University Munich, Department of Surgery, Munich, Germany.
GMS Krankenhhyg Interdiszip. 2007 Dec 28;2(2):Doc53.
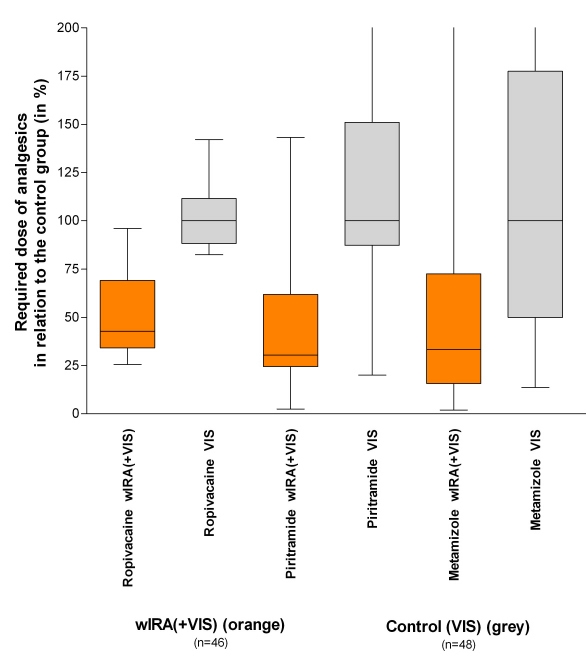
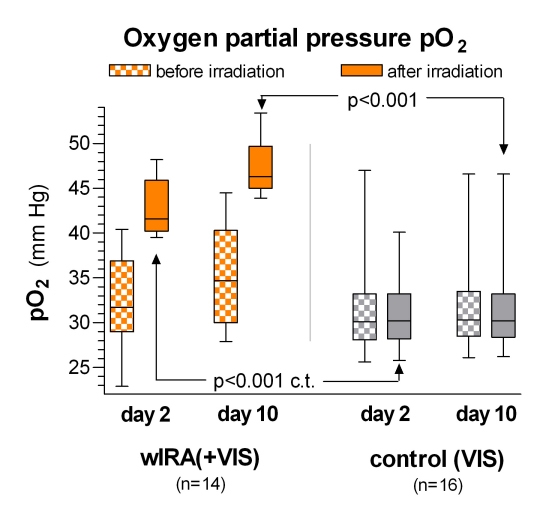
Water-filtered infrared-A (wIRA) as a special form of heat radiation with a high tissue penetration and with a low thermal load to the skin surface acts both by thermal and thermic as well as by non-thermal and non-thermic effects. wIRA produces a therapeutically usable field of heat in the tissue and increases tissue temperature, tissue oxygen partial pressure, and tissue perfusion. These three factors are decisive for a sufficient tissue supply with energy and oxygen and consequently as well for wound healing and infection defense. wIRA can considerably alleviate the pain (with remarkably less need for analgesics) and diminish an elevated wound exudation and inflammation and can show positive immunomodulatory effects. wIRA can advance wound healing or improve an impaired wound healing both in acute and in chronic wounds including infected wounds. Even the normal wound healing process can be improved.A prospective, randomized, controlled, double-blind study with 111 patients after major abdominal surgery at the University Hospital Heidelberg, Germany, showed with 20 minutes irradiation twice a day (starting on the second postoperative day) in the group with wIRA and visible light VIS (wIRA(+VIS), approximately 75% wIRA, 25% VIS) compared to a control group with only VIS a significant and relevant pain reduction combined with a markedly decreased required dose of analgesics: during 230 single irradiations with wIRA(+VIS) the pain decreased without any exception (median of decrease of pain on postoperative days 2-6 was 13.4 on a 100 mm visual analog scale VAS 0-100), while pain remained unchanged in the control group (p<0.001). The required dose of analgesics was 57-70% lower in the subgroups with wIRA(+VIS) compared to the control subgroups with only VIS (median 598 versus 1398 ml ropivacaine, p<0.001, for peridural catheter analgesia; 31 versus 102 mg piritramide, p=0.001, for patient-controlled analgesia; 3.4 versus 10.2 g metamizole, p=0.005, for intravenous and oral analgesia). During irradiation with wIRA(+VIS) the subcutaneous oxygen partial pressure rose markedly by approximately 30% and the subcutaneous temperature by approximately 2.7 degrees C (both in a tissue depth of 2 cm), whereas both remained unchanged in the control group: after irradiation the median of the subcutaneous oxygen partial pressure was 41.6 (with wIRA) versus 30.2 mm Hg in the control group (p<0.001), the median of the subcutaneous temperature was 38.9 versus 36.4 degrees C (p<0.001). The overall evaluation of the effect of irradiation, including wound healing, pain and cosmesis, assessed on a VAS (0-100 with 50 as indifferent point of no effect) by the surgeon (median 79.0 versus 46.8, p<0.001) or the patient (79.0 versus 50.2, p<0.001) was markedly better in the group with wIRA compared to the control group. This was also true for single aspects: Wound healing assessed on a VAS by the surgeon (median 88.6 versus 78.5, p<0.001) or the patient (median 85.8 versus 81.0, p=0.040, trend) and cosmetic result assessed on a VAS by the surgeon (median 84.5 versus 76.5, p<0.001) or the patient (median 86.7 versus 73.6, p=0.001). In addition there was a trend in favor of the wIRA group to a lower rate of total wound infections (3 of 46, approximately 7%, versus 7 of 48, approximately 15%, p=0.208) including late infections after discharge, caused by the different rate of late infections after discharge: 0 of 46 in the wIRA group and 4 of 48 in the control group. And there was a trend towards a shorter postoperative hospital stay: 9 days in the wIRA group versus 11 days in the control group (p=0.037). The principal finding of this study was that postoperative irradiation with wIRA can improve even a normal wound healing process.A prospective, randomized, controlled, double-blind study with 45 severely burned children at the Children's Hospital Park Schönfeld, Kassel, Germany, showed with 30 minutes irradiation once a day (starting on the first day, day of burn as day 1) in the group with wIRA and visible light VIS (wIRA(+VIS), approximately 75% wIRA, 25% VIS) compared to a control group with only VIS a markedly faster reduction of wound size. On the fifth day (after 4 days with irradiation) decision was taken, whether surgical debridement of necrotic tissue was necessary because of deeper (second degree, type b) burns (11 of 21 in the group with wIRA, 14 of 24 in the control group) or non-surgical treatment was possible (second degree, type a, burns). The patients treated conservatively were kept within the study and irradiated till complete reepithelialization. The patients in the group with wIRA showed a markedly faster reduction of wound area: a median reduction of wound size of 50% was reached already after 7 days compared to 9 days in the control group, a median reduction of wound size of 90% was already achieved after 9 days compared to 13 days in the control group. In addition the group with wIRA showed superior results till 3 months after the burn in terms of the overall surgical assessment of the wound, cosmesis, and assessment of effects of irradiation compared to the control group. In a prospective, randomized, controlled study with 12 volunteers at the University Medical Center Charité, Berlin, Germany, within each volunteer 4 experimental superficial wounds (5 mm diameter) as an acute wound model were generated by suction cup technique, removing the roof of the blister with a scalpel and a sterile forceps (day 1). 4 different treatments were used and investigated during 10 days: no therapy, only wIRA(+VIS) (approximately 75% wIRA, 25% VIS; 30 minutes irradiation once a day), only dexpanthenol (= D-panthenol) cream once a day, wIRA(+VIS) and dexpanthenol cream once a day. Healing of the small experimental wounds was from a clinical point of view excellent with all 4 treatments. Therefore there were only small differences between the treatments with slight advantages of the combination wIRA(+VIS) and dexpanthenol cream and of dexpanthenol cream alone concerning relative change of wound size and assessment of feeling of the wound area. However laser scanning microscopy with a scoring system revealed differences between the 4 treatments concerning the formation of the stratum corneum (from first layer of corneocytes to full formation) especially on the days 5-7: fastest formation of the stratum corneum was seen in wounds treated with wIRA(+VIS) and dexpanthenol cream, second was wIRA(+VIS) alone, third dexpanthenol cream alone and last were untreated wounds. Bacterial counts of the wounds (taken every 2 days) showed, that wIRA(+VIS) and the combination of wIRA(+VIS) with dexpanthenol cream were able to inhibit the colonisation with physiological skin flora up to day 5 when compared with the two other groups (untreated group and group with dexpanthenol cream alone). At any investigated time, the amount of colonisation under therapy with wIRA(+VIS) alone was lower (interpreted as more suppressed) compared with the group with wIRA(+VIS) and dexpanthenol cream. During rehabilitation after hip and knee endoprosthetic operations the resorption of wound seromas and wound hematomas was both clinically and sonographically faster and pain was reduced by irradiation with wIRA(+VIS). wIRA can be used successfully for persistent postoperative pain e.g. after thoracotomy.As perspectives for wIRA it seems clinically prudent to use wIRA both pre- and postoperatively, e.g. in abdominal and thoracic operations. wIRA can be used preoperatively (e.g. during 1-2 weeks) to precondition donor and recipient sites of skin flaps, transplants or partial-thickness skin grafts, and postoperatively to improve wound healing and to decrease pain, inflammation and infections at all mentioned sites. wIRA can be used to support routine pre- or intraoperative antibiotic administration or it might even be discussed to replace this under certain conditions by wIRA.
水过滤红外-A(wIRA)作为一种特殊形式的热辐射,具有高组织穿透性且对皮肤表面热负荷低,通过热效应和非热效应发挥作用。wIRA在组织中产生治疗可用的热场,并提高组织温度、组织氧分压和组织灌注。这三个因素对于组织获得充足的能量和氧气供应,进而对于伤口愈合和抗感染至关重要。wIRA可显著减轻疼痛(对镇痛药的需求显著减少),减少伤口渗出和炎症,并具有积极的免疫调节作用。wIRA可促进急性和慢性伤口(包括感染伤口)的伤口愈合或改善受损的伤口愈合。甚至正常的伤口愈合过程也可得到改善。德国海德堡大学医院对111例腹部大手术后患者进行的一项前瞻性、随机、对照、双盲研究表明,与仅接受可见光(VIS)的对照组相比,wIRA与可见光VIS联合治疗组(wIRA(+VIS),约75% wIRA,25% VIS)每天照射两次,每次20分钟(术后第二天开始),疼痛显著减轻,所需镇痛药剂量明显减少:在230次wIRA(+VIS)单次照射期间,疼痛无一例外减轻(术后第2 - 6天疼痛减轻的中位数在100 mm视觉模拟量表VAS 0 - 100上为13.4),而对照组疼痛无变化(p<0.0