Center for Systems Biology, Michigan State University, East Lansing, Michigan, USA.
PLoS One. 2010 Apr 2;5(4):e10031. doi: 10.1371/journal.pone.0010031.
Network analysis has been performed on large-scale medical data, capturing the global topology of drugs, targets, and disease relationships. A smaller-scale network is amenable to a more detailed and focused analysis of the individual members and their interactions in a network, which can complement the global topological descriptions of a network system. Analysis of these smaller networks can help address questions, i.e., what governs the pairing of the different cancers and drugs, is it driven by molecular findings or other factors, such as death statistics.
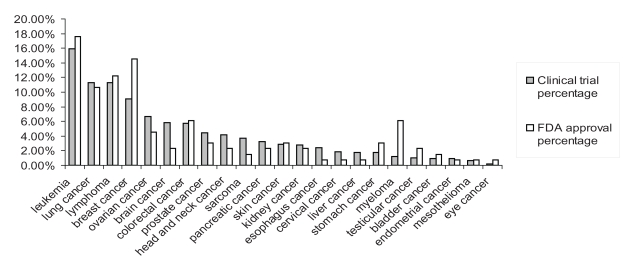
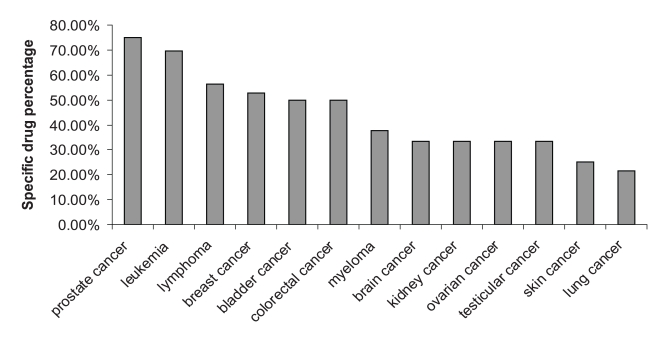
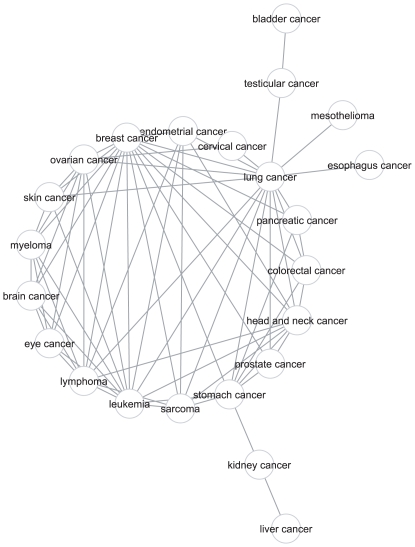
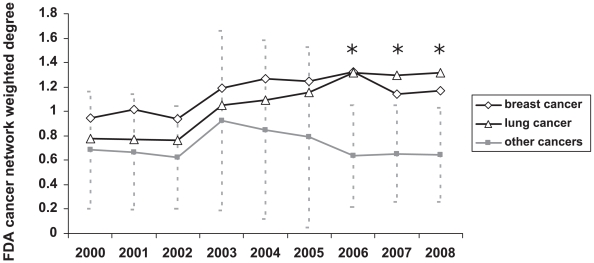
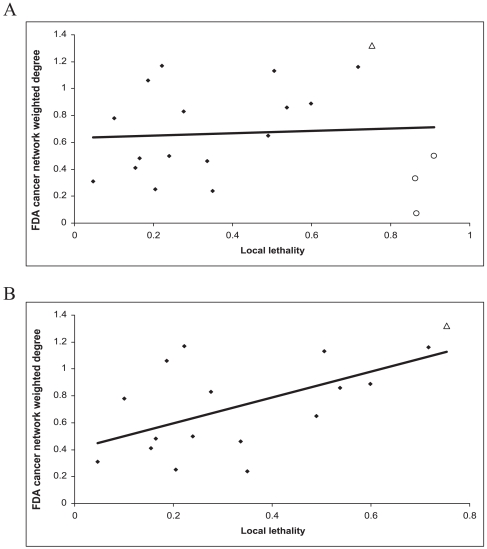
METHODOLOGY/PRINCIPAL FINDINGS: We defined global and local lethality values representing death rates relative to other cancers vs. within a cancer. We generated two cancer networks, one of cancer types that share Food and Drug Administration (FDA) approved drugs (FDA cancer network), and another of cancer types that share clinical trials of FDA approved drugs (clinical trial cancer network). Breast cancer is the only cancer type with significant weighted degree values in both cancer networks. Lung cancer is significantly connected in the FDA cancer network, whereas ovarian cancer and lymphoma are significantly connected in the clinical trial cancer network. Correlation and linear regression analyses showed that global lethality impacts the drug approval and trial numbers, whereas, local lethality impacts the amount of drug sharing in trials and approvals. However, this effect does not apply to pancreatic, liver, and esophagus cancers as the sharing of drugs for these cancers is very low. We also collected mutation target information to generate cancer type associations which were compared with the cancer type associations derived from the drug target information. The analysis showed a weak overlap between the mutation and drug target based networks.
CONCLUSIONS/SIGNIFICANCE: The clinical and FDA cancer networks are differentially connected, with only breast cancer significantly connected in both networks. The networks of cancer-drug associations are moderately affected by the death statistics. A strong overlap does not exist between the cancer-drug associations and the molecular information. Overall, this analysis provides a systems level view of cancer drugs and suggests that death statistics (i.e. global vs. local lethality) have a differential impact on the number of approvals, trials and drug sharing.
已对大规模医学数据进行了网络分析,以捕获药物、靶点和疾病关系的全局拓扑结构。较小规模的网络更适合对网络中的各个成员及其相互作用进行更详细和集中的分析,从而可以补充网络系统的全局拓扑描述。对这些较小网络的分析可以帮助解决问题,例如,不同癌症和药物的配对是由分子发现还是其他因素(例如死亡统计数据)驱动的。
方法/主要发现:我们定义了全局和局部致死值,分别代表相对于其他癌症的死亡率和癌症内部的死亡率。我们生成了两个癌症网络,一个是具有美国食品和药物管理局 (FDA) 批准药物的癌症类型网络(FDA 癌症网络),另一个是具有 FDA 批准药物临床试验的癌症类型网络(临床试验癌症网络)。乳腺癌是两个癌症网络中均具有显著加权度值的唯一癌症类型。肺癌在 FDA 癌症网络中连接显著,而卵巢癌和淋巴瘤在临床试验癌症网络中连接显著。相关性和线性回归分析表明,全局致死率影响药物批准和试验数量,而局部致死率影响试验和批准中药物共享的数量。然而,这种效应不适用于胰腺癌、肝癌和食管癌,因为这些癌症的药物共享非常低。我们还收集了突变靶点信息来生成癌症类型关联,并将其与从药物靶点信息中得出的癌症类型关联进行比较。分析表明,突变和药物靶点的网络之间存在微弱的重叠。
结论/意义:临床和 FDA 癌症网络连接方式不同,只有乳腺癌在两个网络中均连接显著。癌症-药物关联网络受到死亡统计数据的中度影响。癌症-药物关联与分子信息之间没有很强的重叠。总体而言,这项分析提供了癌症药物的系统水平视图,并表明死亡统计数据(即全局与局部致死率)对批准数量、试验数量和药物共享具有不同的影响。