Department of Internal Medicine I, Klinikum Saarbrücken, Winterberg 1, D-66119 Saarbrücken, Germany.
Arthritis Res Ther. 2010;12(3):R79. doi: 10.1186/ar3002. Epub 2010 May 10.
The efficacy and the optimal type and volume of aerobic exercise (AE) in fibromyalgia syndrome (FMS) are not established. We therefore assessed the efficacy of different types and volumes of AE in FMS.
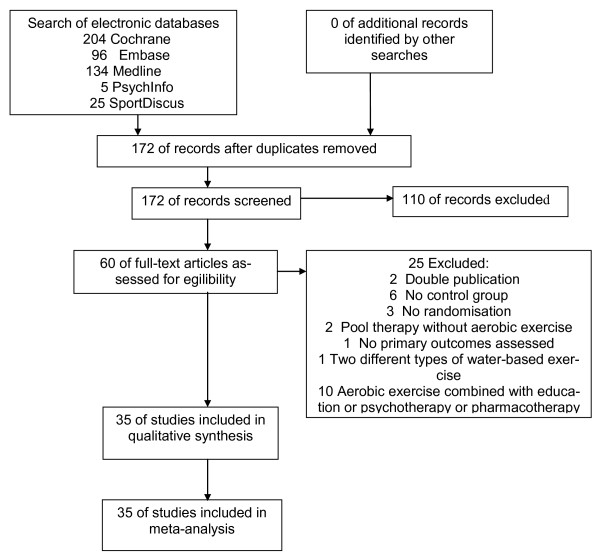
The Cochrane Library, EMBASE, MEDLINE, PsychInfo and SPORTDISCUS (through April 2009) and the reference sections of original studies and systematic reviews on AE in FMS were systematically reviewed. Randomised controlled trials (RCTs) of AE compared with controls (treatment as usual, attention placebo, active therapy) and head-to-head comparisons of different types of AE were included. Two authors independently extracted articles using predefined data fields, including study quality indicators.
Twenty-eight RCTs comparing AE with controls and seven RCTs comparing different types of AE with a total of 2,494 patients were reviewed. Effects were summarised using standardised mean differences (95% confidence intervals) by random effect models. AE reduced pain (-0.31 (-0.46, -0.17); P<0.001), fatigue (-0.22 (-0.38, -0.05); P=0.009), depressed mood (-0.32 (-0.53, -0.12); P=0.002) and limitations of health-related quality of life (HRQOL) (-0.40 (-0.60, -0.20); P<0.001), and improved physical fitness (0.65 (0.38, 0.95); P<0.001), post treatment. Pain was significantly reduced post treatment by land-based and water-based AE, exercises with slight to moderate intensity and frequency of two or three times per week. Positive effects on depressed mood, HRQOL and physical fitness could be maintained at follow-up. Continuing exercise was associated with positive outcomes at follow-up. Risks of bias analyses did not change the robustness of the results. Few studies reported a detailed exercise protocol, thus limiting subgroup analyses of different types of exercise.
An aerobic exercise programme for FMS patients should consist of land-based or water-based exercises with slight to moderate intensity two or three times per week for at least 4 weeks. The patient should be motivated to continue exercise after participating in an exercise programme.
在纤维肌痛综合征(FMS)中,有氧运动(AE)的疗效和最佳类型和量尚不确定。因此,我们评估了不同类型和量的 AE 在 FMS 中的疗效。
系统检索了 Cochrane 图书馆、EMBASE、MEDLINE、PsychInfo 和 SPORTDISCUS(截至 2009 年 4 月)以及关于 FMS 中 AE 的原始研究和系统评价的参考文献部分。包括与对照组(常规治疗、安慰剂对照、积极治疗)比较的 AE 的随机对照试验(RCT)以及不同类型的 AE 之间的头对头比较。两名作者使用预定义的数据字段独立提取文章,包括研究质量指标。
共综述了 28 项比较 AE 与对照组的 RCT 和 7 项比较不同类型 AE 的 RCT,共 2494 名患者。使用随机效应模型汇总了标准化均数差(95%置信区间)的效应。AE 降低了疼痛(-0.31(-0.46,-0.17);P<0.001)、疲劳(-0.22(-0.38,-0.05);P=0.009)、抑郁情绪(-0.32(-0.53,-0.12);P=0.002)和健康相关生活质量(HRQOL)的限制(-0.40(-0.60,-0.20);P<0.001),并改善了体能(0.65(0.38,0.95);P<0.001),治疗后。陆地和水上有氧运动、低至中等强度的运动以及每周两次或三次的运动频率显著降低了治疗后的疼痛。对抑郁情绪、HRQOL 和身体状况的积极影响可以在随访中维持。继续锻炼与随访中的积极结果相关。偏倚风险分析并没有改变结果的稳健性。很少有研究报告了详细的锻炼方案,因此限制了不同类型锻炼的亚组分析。
FMS 患者的有氧运动方案应包括低至中等强度的陆地或水上运动,每周两次或三次,至少持续 4 周。患者应在参加运动方案后有动力继续锻炼。