Bischoff Andrea, Levitt Marc A, Lawal Taiwo A, Peña Alberto
Division of Pediatric Surgery, Colorectal Center for Children, Cincinnati Children's Hospital Medical Center, 3333 Burnet Avenue, ML 2023, Cincinnati, OH 45229, USA.
Pediatr Surg Int. 2010 Nov;26(11):1087-92. doi: 10.1007/s00383-010-2690-6.
Colostomy is an operation frequently performed in pediatric surgery. Despite its benefits, it can produce significant morbidity. In a previous publication we presented our experience with the errors and complications that occurred during cases of colostomy creation. We now have focused in the morbidity related to the colostomy closure. The technical details that might have contributed to the minimal morbidity we experienced are described.
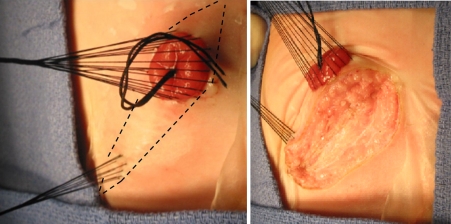
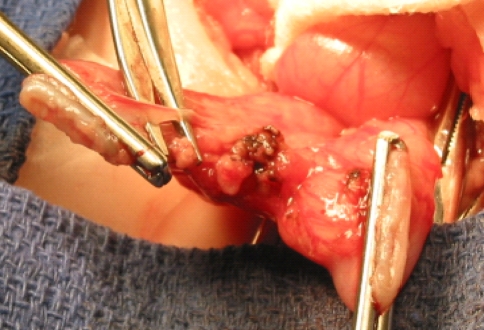
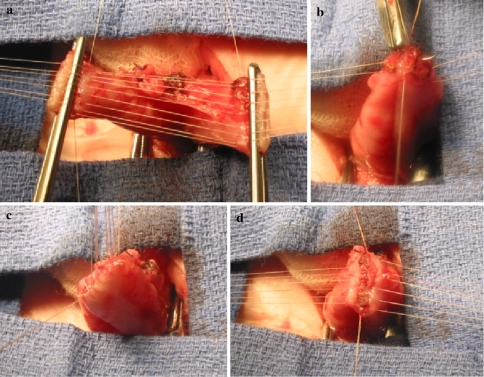
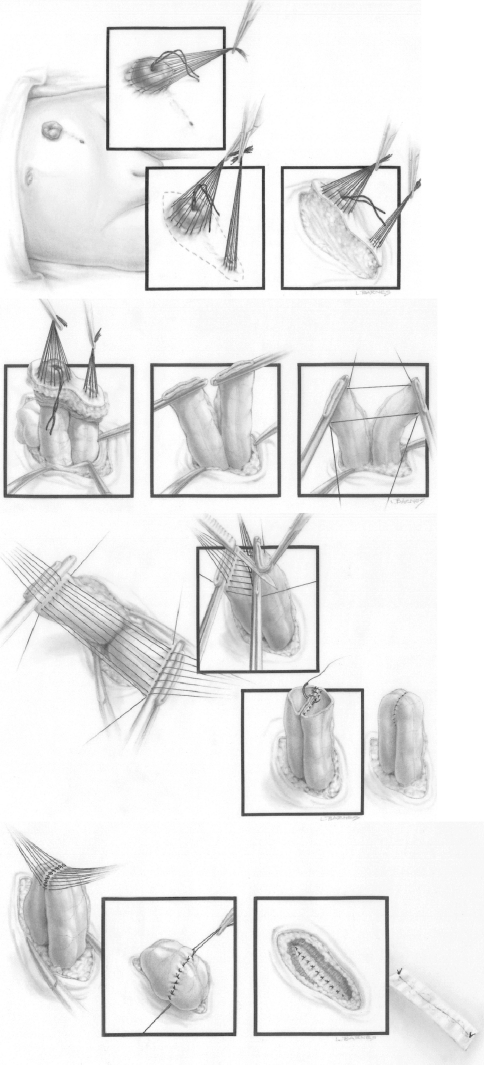
The medical records of 649 patients who underwent colostomy closure over a 28-year period were retrospectively reviewed looking for complications following these procedures. Our perioperative protocol for colostomy closure consisted in: clear fluids by mouth and repeated proximal stoma irrigations 24 h prior to the operation. Administration of IV antibiotics during anesthesia induction and continued for 48 h. Meticulous surgical technique that included: packing of the proximal stoma, plastic drape to immobilize the surgical field, careful hemostasis, emphasis in avoiding contamination, cleaning the edge of the stomas to allow a good 2-layer, end-to-end anastomosis with separated long-term absorbable sutures, generous irrigation of the peritoneal cavity and subsequent layers with saline solution, closure by layers to avoid dead space, and avoidance of hematomas. No drains and no nasogastric tubes were used. Oral fluids were started the day after surgery and patients were discharged 48-72 h after the operation.
The original diagnoses of the patients were: anorectal malformation (583), Hirschsprung's disease (53), and others (13). 10 patients (1.5%) had complications: 6 had intestinal obstruction (5 due to small bowel adhesions, 1 had temporary delay of the function of the anastomosis due to a severe size discrepancy between proximal and distal stoma with a distal microcolon) and 4 incisional hernias. There were no anastomotic dehiscences or wound infection. There was no bleeding, no anastomotic stricture and no mortality.
Based on this experience we believe that colostomy closure can be performed with minimal morbidity provided a meticulous technique is observed.
结肠造口术是小儿外科中经常施行的手术。尽管有其益处,但它会引发显著的发病率。在之前的一篇出版物中,我们介绍了我们在结肠造口术创建病例中所遇到的失误和并发症的经验。我们现在关注的是与结肠造口关闭相关的发病率。描述了可能导致我们所经历的最低发病率的技术细节。
回顾性分析了649例在28年期间接受结肠造口关闭术的患者的病历,以查找这些手术后的并发症。我们的结肠造口关闭围手术期方案包括:术前24小时经口给予清流食并反复冲洗近端造口。麻醉诱导期间静脉给予抗生素并持续48小时。采用细致的手术技术,包括:填塞近端造口、使用塑料单固定手术区域、仔细止血、强调避免污染、清洁造口边缘以进行良好的两层端端吻合,使用可长期吸收的缝线分开缝合、用盐溶液充分冲洗腹腔及后续各层、分层缝合以避免死腔、避免形成血肿。未使用引流管和鼻胃管。术后第一天开始经口进食,患者在术后48 - 72小时出院。
患者的初始诊断为:肛门直肠畸形(583例)、先天性巨结肠(53例)和其他(13例)。10例患者(1.5%)出现并发症:6例发生肠梗阻(5例因小肠粘连,1例因近端和远端造口严重尺寸差异且远端为小结肠导致吻合口功能暂时延迟)和4例切口疝。无吻合口裂开或伤口感染。无出血、无吻合口狭窄且无死亡病例。
基于此经验,我们认为只要遵循细致的技术,结肠造口关闭术可以以最低的发病率进行。