Department of Cardiology, Copenhagen University Hospital Gentofte, Hellerup, Denmark.
Cardiovasc Diabetol. 2010 Sep 16;9:54. doi: 10.1186/1475-2840-9-54.
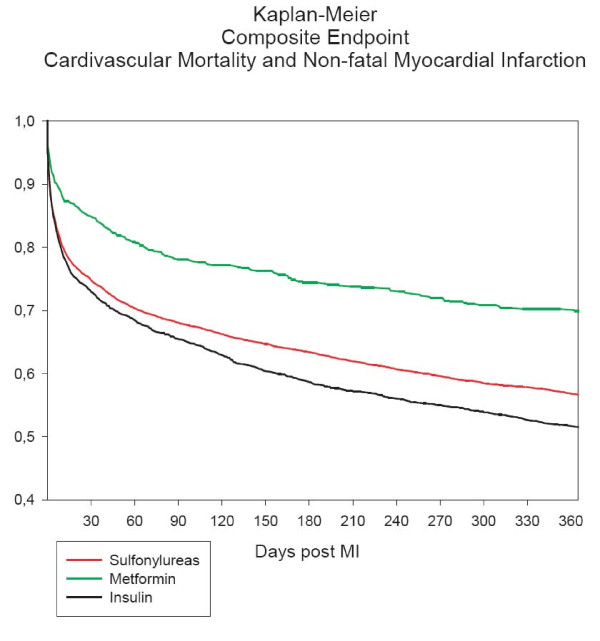
The optimum oral pharmacological treatment of diabetes mellitus to reduce cardiovascular disease and mortality following myocardial infarction has not been established. We therefore set out to investigate the association between individual oral glucose-lowering drugs and cardiovascular outcomes following myocardial infarction in patients with diabetes mellitus not treated with emergent percutaneous coronary intervention.
All patients aged 30 years or older receiving glucose-lowering drugs (GLDs) and admitted with myocardial infarction (MI) not treated with emergent percutaneous coronary intervention in Denmark during 1997-2006 were identified by individual-level linkage of nationwide registries of hospitalizations and drug dispensing from pharmacies. Multivariable Cox regression models adjusted for age, sex, calendar year, comorbidity, and concomitant pharmacotherapy were used to assess differences in the composite endpoint of non-fatal MI and cardiovascular mortality between individual GLDs, using metformin monotherapy as reference.
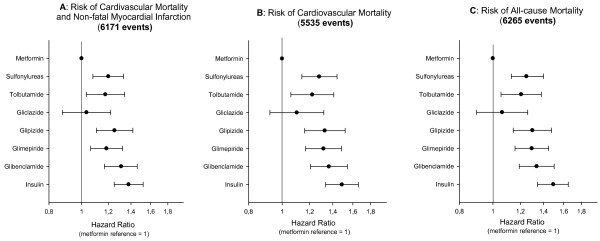
The study comprised 9876 users of GLDs admitted with MI. The mean age was 72.3 years and 56.5% of patients were men. A total of 3649 received sulfonylureas and 711 received metformin at admission. The average length of follow-up was 2.2 (SD 2.6) years. A total of 6,171 patients experienced the composite study endpoint. The sulfonylureas glibenclamide, glimepiride, glipizide, and tolbutamide were associated with increased risk of cardiovascular mortality and/or nonfatal MI with hazard ratios [HRs] of 1.31 (95% confidence interval [CI] 1.17-1.46), 1.19 (1.06-1.32), 1.25 (1.11-1.42), and 1.18 (1.03-1.34), respectively, compared with metformin. Gliclazide was the only sulfonylurea not associated with increased risk compared with metformin (HR 1.03 [0.88-1.22]).
In patients with diabetes mellitus admitted with MI not treated with emergent percutaneous coronary intervention, monotherapy treatment with the sulfonylureas glibenclamide, glimepiride, glipizide, and tolbutamide was associated with increased cardiovascular risk compared with metformin monotherapy.
为降低心梗后心血管疾病和死亡率,尚未明确最佳的口服降血糖药物治疗糖尿病方案。因此,我们旨在研究心梗后未行紧急经皮冠状动脉介入治疗的糖尿病患者中,不同口服降糖药物与心血管结局的相关性。
通过全国范围内住院和药房配药登记系统的个体水平链接,确定了 1997 年至 2006 年丹麦年龄在 30 岁及以上、接受降糖药物(GLD)治疗且未行紧急经皮冠状动脉介入治疗的心梗患者。多变量 Cox 回归模型调整了年龄、性别、日历年份、合并症和伴随药物治疗,以评估个体 GLD 治疗的非致死性心梗和心血管死亡率复合终点的差异,以二甲双胍单药治疗为参照。
本研究纳入了 9876 名接受 GLD 治疗且因心梗入院的患者。平均年龄为 72.3 岁,56.5%为男性。入院时共有 3649 名患者接受磺酰脲类药物治疗,711 名患者接受二甲双胍治疗。平均随访时间为 2.2(SD 2.6)年。共有 6171 名患者发生复合研究终点事件。磺酰脲类药物格列本脲、格列美脲、格列吡嗪和甲苯磺丁脲的心血管死亡率和/或非致死性心梗风险比(HRs)分别为 1.31(95%置信区间 [CI] 1.17-1.46)、1.19(1.06-1.32)、1.25(1.11-1.42)和 1.18(1.03-1.34),与二甲双胍相比。格列齐特是唯一与二甲双胍相比未增加风险的磺酰脲类药物(HR 1.03 [0.88-1.22])。
心梗后未行紧急经皮冠状动脉介入治疗的糖尿病患者中,与二甲双胍单药治疗相比,格列本脲、格列美脲、格列吡嗪和甲苯磺丁脲单药治疗的磺酰脲类药物与心血管风险增加相关。