Department of Internal Medicine D, Tel-Aviv Sourasky Medical Center and the Sackler Faculty of Medicine, Tel-Aviv University, Tel-Aviv, Israel.
BMC Infect Dis. 2010 Oct 4;10:288. doi: 10.1186/1471-2334-10-288.
Data for predicting which patients with pandemic influenza A (H1N1) infection are likely to run a complicated course are sparse. We retrospectively studied whether the admission serum C-reactive protein (CRP) levels can serve as a predictor of illness severity.
Included were all consecutive adult patients who presented to the emergency department (ED) between May-December, 2009 with a flu-like illness, a confirmed diagnosis of pandemic influenza A (H1N1) infection and a serum CRP level measured within 24 hours of presentation. Patients with a proven additional concurrent acute illness (e.g., bacteremia) were excluded. We used the ROC curve analysis, Kaplan-Meier curves and the Cox proportional hazard model to evaluate the predictive ability of CRP as a prognostic factor.
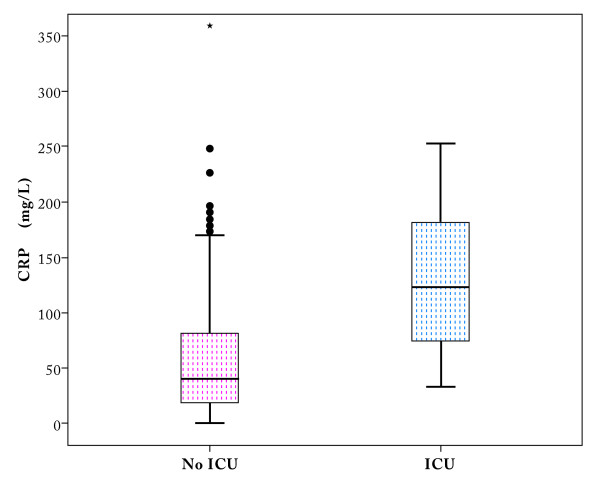
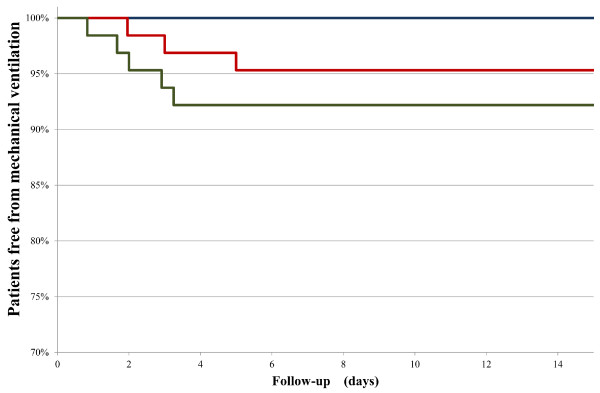
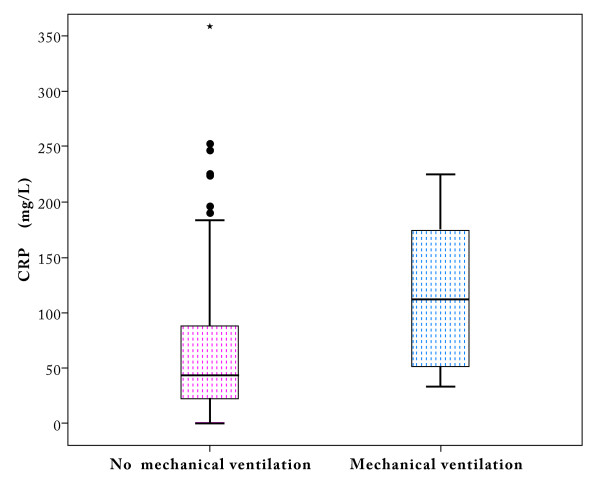
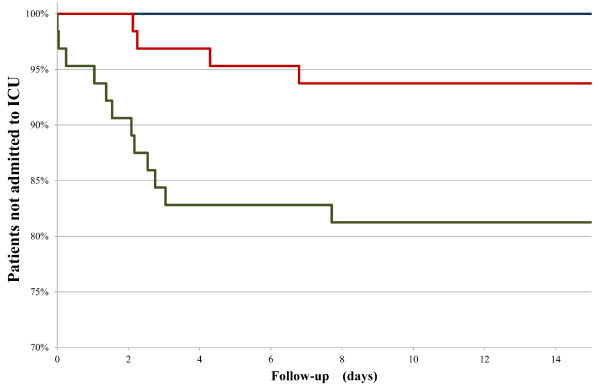
Seventeen (9%) of the 191 enrolled patients were admitted to the intensive care unit (ICU), of whom eight (4%) required mechanical ventilation and three (2%) died. The median admission serum CRP levels were significantly higher among patients who required subsequent ICU care and mechanical ventilation than among patients who did not (123 mg/L and 112 mg/L vs. 40 mg/L, p < .001 and 43 mg/L, p = .017, respectively). A Cox proportional hazard model identified admission serum CRP levels and auscultatory findings over the lungs as independent prognostic factors for ICU admission. Admission serum CRP levels were the only independent prognostic factor for mechanical ventilation. Thirty days after presenting to the ED, none of the patients with admission serum CRP level <28 mg/L (lower tertile) required either ICU admission or mechanical ventilation. At the same time point, 19% of the patients with admission serum CRP level ≥70 mg/L (upper tertile) needed to be admitted to the ICU and 8% of the same upper tertile group required mechanical ventilation. The differences in the rates between the lower vs. upper tertile groups were significant (Log-Rank p < .001 for ICU and p < .024 for mechanical ventilation).
In our study group, serum CRP levels obtained in the early ED admission stage from patients presenting with pandemic H1N1 influenza A infection were found to serve as a useful gauge for predicting disease course and assisting in patient management.
目前对于预测哪些甲型流感(H1N1)感染患者可能出现病情复杂的相关数据较为匮乏。本研究旨在回顾性分析入院时血清 C 反应蛋白(CRP)水平是否可以作为疾病严重程度的预测指标。
连续纳入 2009 年 5 月至 12 月期间因流感样疾病就诊于急诊科、确诊为甲型 H1N1 流感感染且入院 24 小时内检测 CRP 水平的成年患者。排除同时患有明确的其他急性疾病(如菌血症)的患者。采用 ROC 曲线分析、Kaplan-Meier 曲线和 Cox 比例风险模型来评估 CRP 作为预后因素的预测能力。
191 例纳入患者中 17 例(9%)收入重症监护病房(ICU),其中 8 例(4%)需要机械通气,3 例(2%)死亡。需要后续 ICU 治疗和机械通气的患者入院时血清 CRP 中位数明显高于不需要的患者(123mg/L 和 112mg/L 比 40mg/L,p<0.001 和 43mg/L,p=0.017)。Cox 比例风险模型确定入院时血清 CRP 水平和肺部听诊结果为 ICU 入住的独立预后因素。入院时血清 CRP 水平是机械通气的唯一独立预后因素。在急诊科就诊后 30 天,入院时 CRP 水平<28mg/L(下三分之一)的患者无一例需要 ICU 入住或机械通气。同时,入院时 CRP 水平≥70mg/L(上三分之一)的患者中有 19%需要入住 ICU,8%的上三分之一组需要机械通气。下三分之一组与上三分之一组之间的差异有统计学意义(ICU 组 Log-Rank p<0.001,机械通气组 p<0.024)。
在本研究组中,从甲型 H1N1 流感感染患者急诊科早期入院时获得的血清 CRP 水平可作为预测疾病进程和协助患者管理的有用指标。