Service of Neurology, Centre Hospitalier Universitaire Vaudois and University of Lausanne, Switzerland.
BMC Nephrol. 2010 Oct 16;11:27. doi: 10.1186/1471-2369-11-27.
Chronic kidney disease (CKD) is associated to a higher stroke risk. Anemia is a common consequence of CKD, and is also a possible risk factor for cerebrovascular diseases. The purpose of this study was to examine if anemia and CKD are independent risk factors for mortality after stroke.
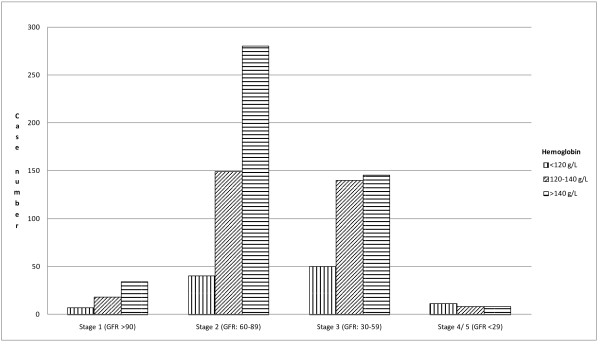
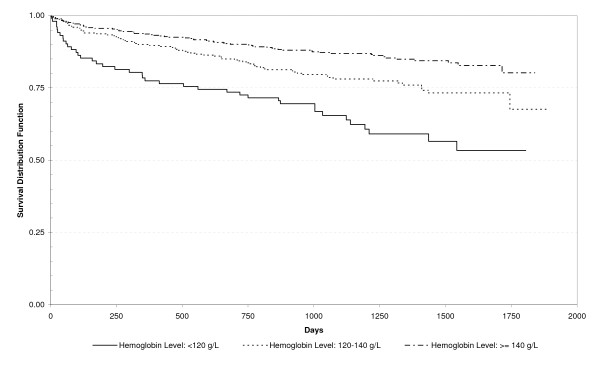
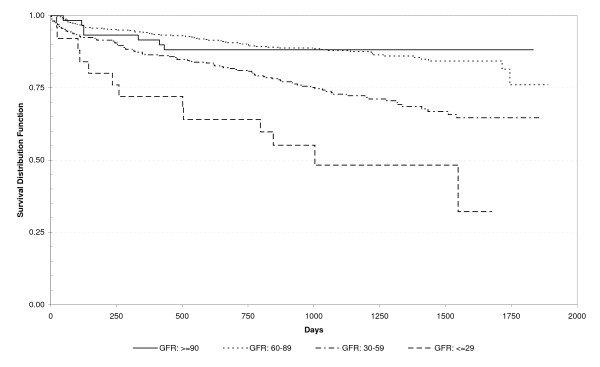
This historic cohort study was based on a stroke registry and included patients treated for a first clinical stroke in the stroke unit of one academic hospital over a three-year period. Mortality predictors comprised demographic characteristics, CKD, glomerular filtration rate (GFR), anemia and other stroke risk factors. GFR was estimated by means of the simplified Modification of Diet in Renal Disease formula. Renal function was assessed according to the Kidney Disease Outcomes Quality Initiative (K/DOQI)-CKD classification in five groups. A value of hemoglobin < 120 g/L in women and < 130 g/L in men on admission defined anemia. Kaplan-Meier survival curves and Cox models were used to describe and analyze one-year survival.
Among 890 adult stroke patients, the mean (Standard Deviation) calculated GFR was 64.3 (17.8) ml/min/1.73 m2 and 17% had anemia. Eighty-two (10%) patients died during the first year after discharge. Among those, 50 (61%) had K/DOQI CKD stages 3 to 5 and 32 (39%) stages 1 or 2 (p < 0.001). Anemia was associated with an increased risk of death one year after discharge (p < 0.001). After adjustment for other factors, a higher hemoglobin level was independently associated with decreased mortality one year after discharge [hazard ratio (95% CI) 0.98 (0.97-1.00)].
Both CKD and anemia are frequent among stroke patients and are potential risk factors for decreased one-year survival. The inclusion of patients with a first-ever clinical stroke only and the determination of anemia based on one single measure, on admission, constitute limitations to the external validity. We should investigate if an early detection and management of both CKD and anemia could improve survival in stroke patients.
慢性肾脏病(CKD)与更高的中风风险相关。贫血是 CKD 的常见后果,也是脑血管疾病的可能危险因素。本研究的目的是检查贫血和 CKD 是否是中风后死亡的独立危险因素。
这是一项基于队列的历史性研究,基于一个中风登记处,包括在一家学术医院中风病房接受首次临床中风治疗的患者,研究时间为三年。死亡率预测因素包括人口统计学特征、CKD、肾小球滤过率(GFR)、贫血和其他中风危险因素。GFR 通过简化肾脏病饮食改良公式估计。根据肾脏病结果质量倡议(K/DOQI)-CKD 分类,肾功能分为五组进行评估。女性血红蛋白<120g/L,男性血红蛋白<130g/L 入院时定义为贫血。采用 Kaplan-Meier 生存曲线和 Cox 模型描述和分析一年生存率。
在 890 名成年中风患者中,计算的平均(标准差)GFR 为 64.3(17.8)ml/min/1.73m2,17%的患者贫血。出院后第一年,82 名(10%)患者死亡。其中,50 名(61%)为 K/DOQI CKD 3 至 5 期,32 名(39%)为 1 或 2 期(p<0.001)。贫血与出院后一年死亡风险增加相关(p<0.001)。在校正其他因素后,较高的血红蛋白水平与出院后一年死亡率降低独立相关[风险比(95%置信区间)0.98(0.97-1.00)]。
中风患者中 CKD 和贫血都很常见,是降低一年生存率的潜在危险因素。仅纳入首次临床中风患者以及基于入院时单一测量值确定贫血存在外推限制。我们应该研究早期发现和管理 CKD 和贫血是否可以改善中风患者的生存率。