Department of Biomedical Science and Human Oncology - Hygiene section, University of Bari, Piazza G. Cesare 11, 70124 Bari, Italy.
BMC Public Health. 2010 Nov 2;10:660. doi: 10.1186/1471-2458-10-660.
Following the publication of the Italian Guidelines for the control and prevention of legionellosis an environmental and clinical surveillance has been carried out in Southeastern Italy. The aim of the study is to identify the risk factors for the disease, so allowing better programming of the necessary prevention measures.
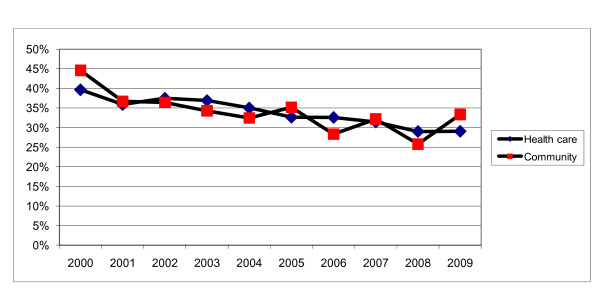
During the period January 2000 - December 2009 the environmental surveillance was carried out by water sampling of 129 health care facilities (73 public and 56 private hospitals) and 533 buildings within the community (63 private apartments, 305 hotels, 19 offices, 4 churches, 116 gyms, 3 swimming pools and 23 schools). Water sampling and microbiological analysis were carried out following the Italian Guidelines. From January 2005, all facilities were subject to risk analysis through the use of a standardized report; the results were classified as good (G), medium (M) and bad (B). As well, all the clinical surveillance forms for legionellosis, which must be compiled by physicians and sent to the Regional Centre for Epidemiology (OER), were analyzed.
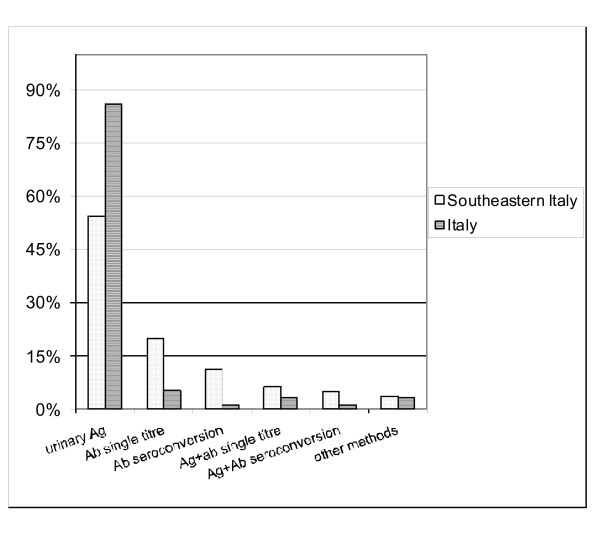
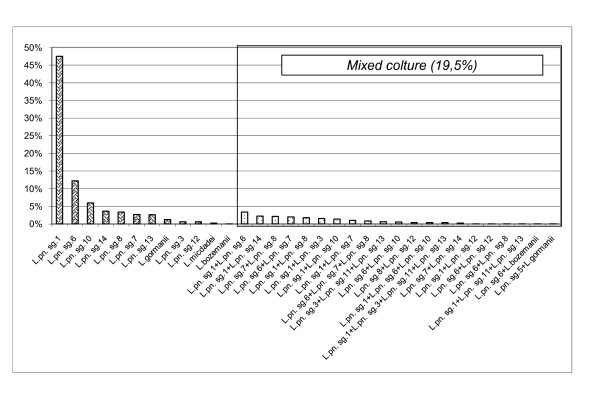
Legionella spp. was found in 102 (79.1%) health care facilities and in 238 (44.7%) community buildings. The percentages for the contamination levels < 1,000, 1,000-10,000, > 10,000 cfu/L were respectively 33.1%, 53.4% and 13.5% for samples from health care facilities and 33.5%, 43.3% and 23.2% for samples from the community. Both in hospital and community environments, Legionella pneumophila serogroup (L. pn sg) 2-14 was the most frequently isolate (respectively 54.8% and 40.8% of positive samples), followed by L. pn sg 1 (respectively 31.3% and 33%). The study showed a significant association between M or B score at the risk analysis and Legionella spp. positive microbiological test results (p < 0.001). From clinical surveillance, during the period January 2001 - August 2009, 97 cases of legionellosis were reported to the OER: 88 of community origin and 9 nosocomial. The most frequent symptoms were: fever (93.8%), cough (70.1%), dyspnea (58.8%), shivering (56.7%). Radiological evidence of pneumonia was reported in 68%. The laboratory diagnostic methods used were: urinary antigen (54.3%), single antibody titer (19.8%), only seroconversion (11.1%), other diagnostic methods (14.8%).
Our experience suggests that risk analysis and environmental microbiological surveillance should be carried out more frequently to control the environmental spread of Legionella spp. Furthermore, the laboratory diagnosis of legionellosis cannot be excluded only on the basis of a single negative test: some patients were positive to only one of the diagnostic tests.
意大利军团病控制和预防指南发布后,在意大利东南部进行了环境和临床监测。本研究旨在确定疾病的危险因素,从而更好地规划必要的预防措施。
2000 年 1 月至 2009 年 12 月期间,通过对 129 家医疗保健机构(73 家公立和 56 家私立医院)和社区内的 533 栋建筑物(63 栋私人公寓、305 家酒店、19 间办公室、4 座教堂、116 间健身房、3 个游泳池和 23 所学校)进行水样采集,开展了环境监测。水样采集和微生物学分析均按照意大利指南进行。自 2005 年 1 月起,所有机构均通过使用标准化报告进行风险分析;结果被归类为良好(G)、中等(M)和差(B)。同时,对所有必须由医生填写并发送给地区流行病学中心(OER)的军团病临床监测表进行了分析。
在 102 家(79.1%)医疗保健机构和 238 栋(44.7%)社区建筑中发现了军团菌属。在医疗保健机构水样中,污染水平<1000、1000-10000、>10000cfu/L 的比例分别为 33.1%、53.4%和 13.5%,而在社区水样中,这一比例分别为 33.5%、43.3%和 23.2%。在医院和社区环境中,最常分离到的是嗜肺军团菌血清群(L. pn sg)2-14(阳性样本分别为 54.8%和 40.8%),其次是 L. pn sg 1(阳性样本分别为 31.3%和 33%)。研究表明,风险分析中的 M 或 B 评分与军团菌属阳性微生物检测结果之间存在显著关联(p<0.001)。从临床监测来看,2001 年 1 月至 2009 年 8 月,向 OER 报告了 97 例军团病病例:9 例为社区感染,88 例为医院感染。最常见的症状是:发热(93.8%)、咳嗽(70.1%)、呼吸困难(58.8%)、寒战(56.7%)。68%的患者有肺炎的放射学证据。使用的实验室诊断方法有:尿抗原(54.3%)、单抗体滴度(19.8%)、仅血清转化(11.1%)、其他诊断方法(14.8%)。
我们的经验表明,应更频繁地进行风险分析和环境微生物监测,以控制军团菌属在环境中的传播。此外,不能仅基于单次阴性检测来排除军团病的实验室诊断:一些患者仅对一种诊断检测呈阳性。