Department of Medicine, The University of Hong Kong, Queen Mary Hospital, Hong Kong, China.
Osteoporos Int. 2011 Nov;22(11):2799-807. doi: 10.1007/s00198-010-1490-0. Epub 2011 Jan 14.
This prospective study aimed to determine the risk factors and the 10-year probability of osteoporotic fracture in Southern Chinese men. The findings show substantial population differences in fracture incidence and risk prediction compared to the FRAX(TM) model, and the addition of BMD information to clinical risk factor assessment improved fracture risk prediction in Chinese men.
Clinical risk factors with or without bone mineral density (BMD) measurements are increasingly recognized as reliable predictors of fracture risk. Prospective data on fracture incidence in Asian men remain sparse. This prospective study aimed to determine the risk factors and the 10-year absolute fracture risk in Southern Chinese men.
This is a part of the Hong Kong Osteoporosis Study. One thousand eight hundred ten (1,810) community-dwelling, treatment-naive men aged 50 years or above were evaluated. Baseline demographic characteristics, clinical risk factors and BMD were recorded. Ten-year risk of osteoporotic fracture was calculated using Cox proportional hazards models.
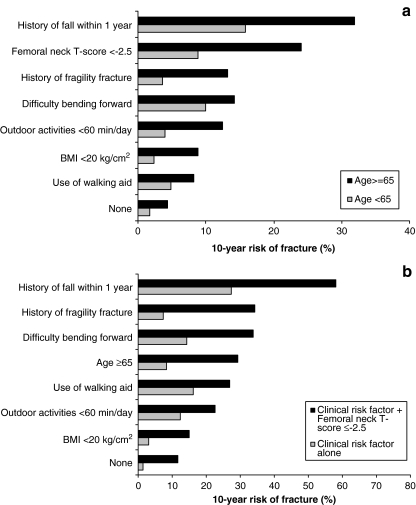
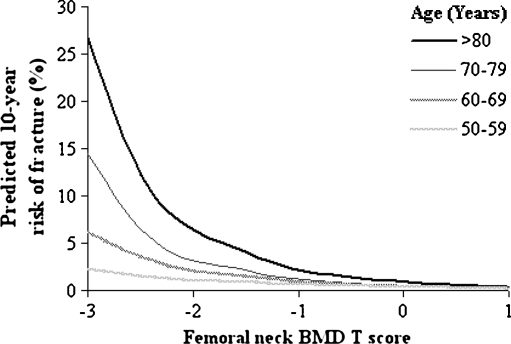
The mean age of subjects was 68.0 ± 10.3 years. After a mean follow-up period of 3.5±2.9 years (range 1 to 14 years), 37 incident low-trauma fractures were recorded. The incidence for all osteoporotic fractures and hip fractures was 635/100,000 and 123/100,000 person-years, respectively. The most significant predictors of osteoporotic fracture were history of fall (RR 14.5), femoral neck BMD T-score < -2.5 (RR 13.8) and history of fracture (RR 4.4). Each SD reduction in BMD was associated with a 1.8 to 2.6-fold increase in fracture risk. Subjects with seven clinical risk factors and BMD T-score of -1 had an absolute 10-year risk of osteoporotic fracture of 8.9%, but this increased to 22.7% if they also had a femoral neck BMD T-score of -2.5.
These findings show substantial population differences in fracture incidence and risk prediction. The addition of BMD information to clinical risk factor assessment improved fracture risk prediction in Chinese men.
本前瞻性研究旨在确定中国南方男性骨质疏松性骨折的危险因素和 10 年骨折发生率。研究结果表明,与 FRAX(TM)模型相比,骨折发生率和风险预测存在显著的人群差异,并且将骨密度信息加入临床危险因素评估可改善中国男性的骨折风险预测。
临床危险因素(无论是否有骨密度测量)越来越被认为是骨折风险的可靠预测指标。亚洲男性骨折发生率的前瞻性数据仍然很少。本前瞻性研究旨在确定中国南方男性的危险因素和 10 年绝对骨折风险。
这是香港骨质疏松症研究的一部分。1810 名(1810 名)居住在社区、未经治疗的 50 岁及以上男性接受了评估。记录了基线人口统计学特征、临床危险因素和骨密度。使用 Cox 比例风险模型计算 10 年骨质疏松性骨折风险。
受试者的平均年龄为 68.0±10.3 岁。在平均 3.5±2.9 年(范围 1 至 14 年)的随访后,记录了 37 例低创伤性骨折事件。所有骨质疏松性骨折和髋部骨折的发生率分别为 635/100,000 和 123/100,000 人年。骨质疏松性骨折的最显著预测因素是既往跌倒史(RR 14.5)、股骨颈骨密度 T 评分< -2.5(RR 13.8)和既往骨折史(RR 4.4)。骨密度每降低 1 个标准差,骨折风险增加 1.8 至 2.6 倍。有 7 项临床危险因素且股骨颈骨密度 T 评分<-1 的患者,10 年骨质疏松性骨折的绝对风险为 8.9%,但如果他们的股骨颈骨密度 T 评分也为-2.5,则风险增加至 22.7%。
这些发现表明,骨折发生率和风险预测存在显著的人群差异。将骨密度信息加入临床危险因素评估可改善中国男性的骨折风险预测。