Mount Sinai Hospital and School of Medicine, Department of Anesthesiology, New York, NY 10029, USA.
Pain Physician. 2011 Jan-Feb;14(1):71-82.
Opioid guidelines recommend opioid rotation and switching for patients who do not achieve adequate pain relief or who experience intolerable adverse events (AEs) with their current opioid. However, specific recommendations and protocols for opioid rotation are lacking, making the practice time consuming and difficult for primary care physicians to accomplish independently or coordinate with a pain specialist.
To assess the safety and feasibility of using 24-hour intravenous patient-controlled analgesia (IV-PCA) to achieve rapid opioid rotation and titration (RORT).
Open-label pilot study.
Hospital research center.
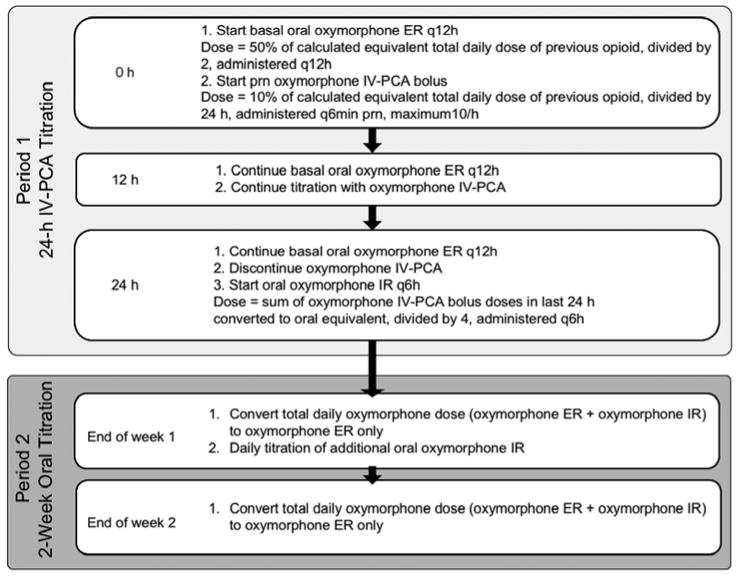
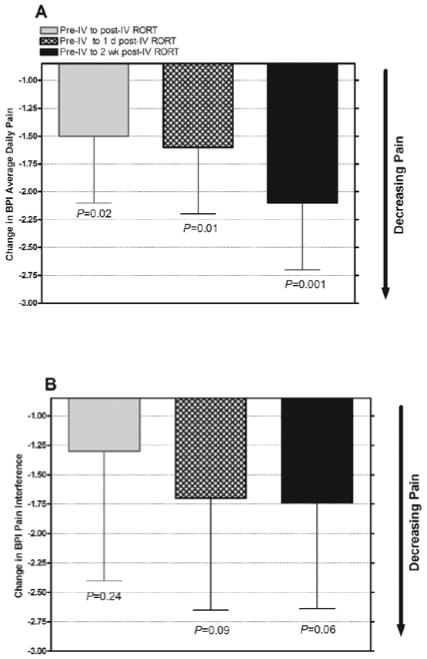
At admission, patients (aged ≥ 18 years) with treatment-refractory chronic pain who were taking morphine or oxycodone for ≥ 3 months and had pain scores ≥ 4 on a 10-point scale, underwent opioid rotation to oral oxymorphone extended release (ER). They also received IV-PCA oxymorphone for 24 hours as needed. At discharge, the participants were taking oral oxymorphone ER with oxymorphone immediate release (IR) as needed based on their total 24-hour oral plus IV-PCA oxymorphone use. During a 2-week follow-up, their oxymorphone usage was titrated as needed. Main outcome measures were AEs, Patient Global Impression of Change (PGIC), Brief Pain Inventory (0 = no pain/interference, 10 = worst pain/complete interference), treatment satisfaction, and change in oxymorphone dose.
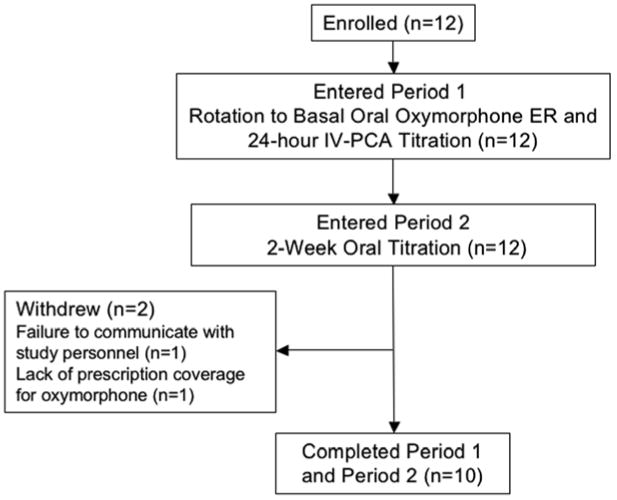
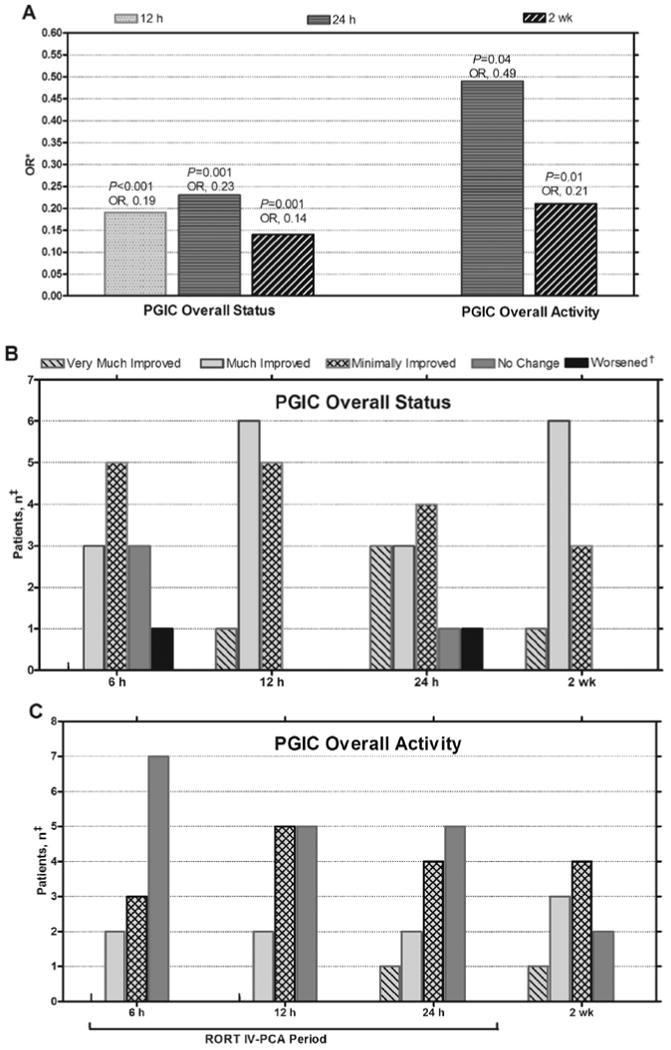
Twelve patients enrolled and completed the 24-hour IV-PCA; 10 completed the 2-week follow-up post-24-hour IV-PCA. PGIC status improved by 12 hours (odds ratio [OR], 0.19, 95% CI, 0.08 - 0.44; P < 0.001), and both PGIC status and activity scores improved by 24 hours (OR, 0.23, 95% CI, 0.09 - 0.55; P = 0.001; OR, 0.49, 95% CI, 0.25 - 0.96; P = 0.04, respectively) and 2 weeks (OR, 0.14, 95% CI, 0.04 - 0.46; P = 0.001; OR, 0.21, 95% CI, 0.06 - 0.72; P = 0.01) versus 6 hours. During the 24-hour IV-PCA time period, 6 of 10 patients accomplished ≥ 50% of their overall dose titration. At 2 weeks, 8 of 10 participants were Greatly Satisfied or Somewhat Satisfied with the overall RORT procedure. RORT was well tolerated, with no serious AEs.
This was a pilot open-label study in a small number of participants. A larger randomized study with long-term follow-up and comparison to traditional protocols is necessary.
Preliminary data suggest that RORT can be performed safely and effectively by incorporating IV-PCA during the first 24 hours. Further investigations are needed to determine whether RORT can become an ambulatory treatment intervention in pain practice.
阿片类药物指南建议对未达到充分疼痛缓解或出现不可耐受不良反应(AE)的患者进行阿片类药物的转换和切换。然而,缺乏具体的阿片类药物转换和切换建议和方案,这使得初级保健医生难以独立完成或与疼痛专家协调。
评估使用 24 小时静脉患者自控镇痛(IV-PCA)实现快速阿片类药物转换和滴定(RORT)的安全性和可行性。
开放标签的初步研究。
医院研究中心。
入院时,患有治疗抵抗性慢性疼痛的患者(年龄≥18 岁),接受吗啡或羟考酮治疗≥3 个月,疼痛评分≥10 分制的 4 分,接受口服奥沙吗啡缓释片(ER)的阿片类药物转换。他们还按需接受 24 小时 IV-PCA 奥沙吗啡。出院时,患者根据其 24 小时口服加 IV-PCA 奥沙吗啡的总用量,开始口服奥沙吗啡 ER 加奥沙吗啡即时释放(IR)。在接下来的 2 周随访期间,根据需要调整奥沙吗啡的用量。主要观察指标为不良事件(AE)、患者整体印象变化(PGIC)、简明疼痛量表(0=无痛/无干扰,10=最痛/完全干扰)、治疗满意度和奥沙吗啡剂量变化。
12 名患者入组并完成了 24 小时 IV-PCA;10 名患者完成了 24 小时 IV-PCA 后的 2 周随访。PGIC 状态在 12 小时内改善(比值比[OR],0.19,95%可信区间,0.08-0.44;P<0.001),PGIC 状态和活动评分在 24 小时内改善(OR,0.23,95%可信区间,0.09-0.55;P=0.001;OR,0.49,95%可信区间,0.25-0.96;P=0.04)和 2 周时改善(OR,0.14,95%可信区间,0.04-0.46;P=0.001;OR,0.21,95%可信区间,0.06-0.72;P=0.01),与 6 小时相比。在 24 小时 IV-PCA 期间,10 名患者中有 6 名完成了总剂量滴定的≥50%。在 2 周时,10 名参与者中有 8 名对整体 RORT 过程非常满意或有些满意。RORT 耐受性良好,无严重 AE。
这是一项小规模患者参与的初步开放标签研究。需要一项更大规模的随机研究,进行长期随访,并与传统方案进行比较。
初步数据表明,通过在最初 24 小时内加入 IV-PCA,RORT 可以安全有效地进行。需要进一步研究以确定 RORT 是否可以成为疼痛治疗中的一种门诊治疗干预措施。