Glaucoma Service, Dana Center for Preventive Ophthalmology, Wilmer Eye Institute, Johns Hopkins University, Baltimore, MD, USA.
BMC Ophthalmol. 2011 Feb 11;11:6. doi: 10.1186/1471-2415-11-6.
The definitive diagnosis of glaucoma is currently based on congruent damage to both optic nerve structure and function. Given widespread quantitative assessment of both structure (imaging) and function (automated perimetry) in glaucoma, it should be possible to combine these quantitative data to diagnose disease. We have therefore defined and tested a new approach to glaucoma diagnosis by combining imaging and visual field data, using the anatomical organization of retinal ganglion cells.
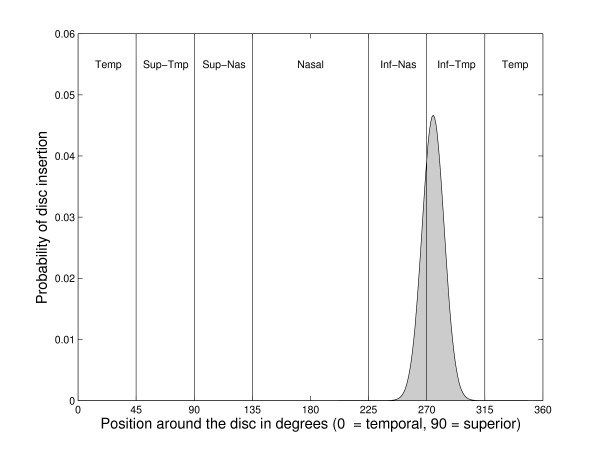
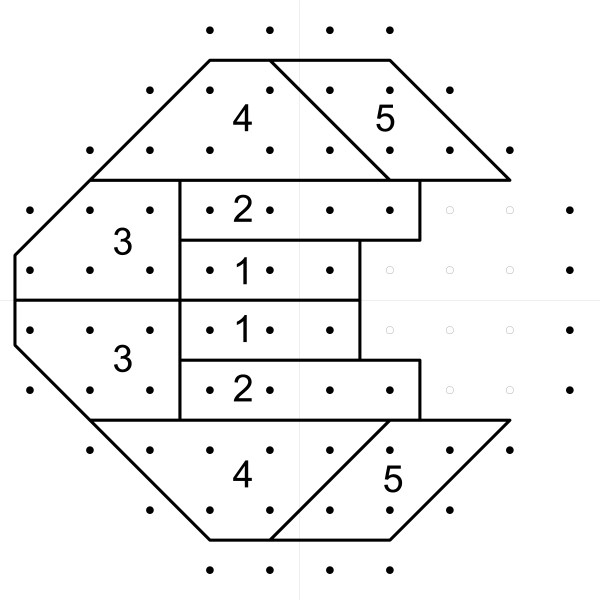
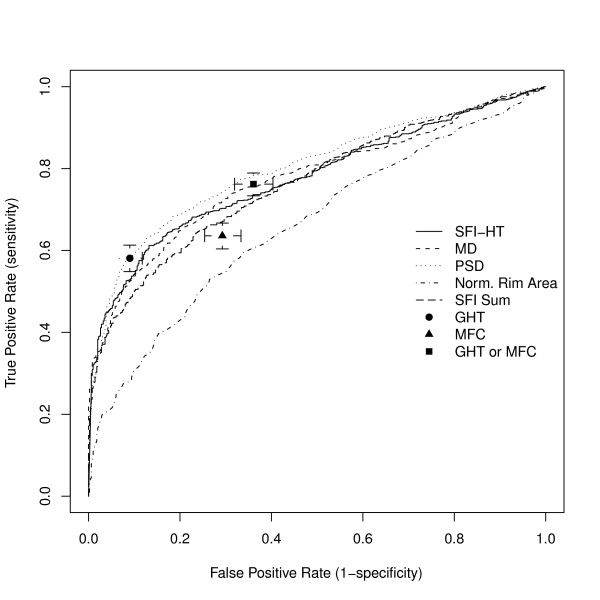
Data from 1499 eyes of glaucoma suspects and 895 eyes with glaucoma were identified at a single glaucoma center. Each underwent Heidelberg Retinal Tomograph (HRT) imaging and standard automated perimetry. A new measure combining these two tests, the structure function index (SFI), was defined in 3 steps: 1) calculate the probability that each visual field point is abnormal, 2) calculate the probability of abnormality for each of the six HRT optic disc sectors, and 3) combine those probabilities with the probability that a field point and disc sector are linked by ganglion cell anatomy. The SFI was compared to the HRT and visual field using receiver operating characteristic (ROC) analysis.
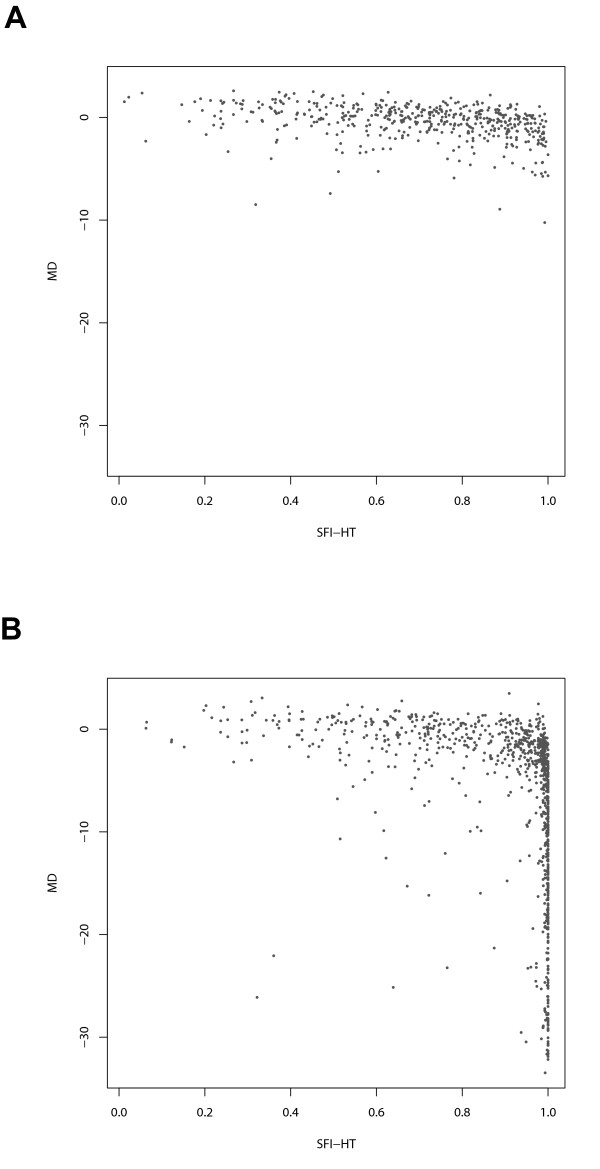
The SFI produced an area under the ROC curve (0.78) that was similar to that for both visual field mean deviation (0.78) and pattern standard deviation (0.80) and larger than that for a normalized measure of HRT rim area (0.66). The cases classified as glaucoma by the various tests were significantly non-overlapping. Based on the distribution of test values in the population with mild disease, the SFI may be better able to stratify this group while still clearly identifying those with severe disease.
The SFI reflects the traditional clinical diagnosis of glaucoma by combining optic nerve structure and function. In doing so, it identifies a different subset of patients than either visual field testing or optic nerve head imaging alone. Analysis of prospective data will allow us to determine whether the combined index of structure and function can provide an improved standard for glaucoma diagnosis.
目前青光眼的明确诊断基于视神经结构和功能的一致性损伤。鉴于青光眼的结构(成像)和功能(自动视野计)的广泛定量评估,应该可以将这些定量数据结合起来诊断疾病。因此,我们通过结合视网膜神经节细胞的解剖结构,定义并测试了一种使用成像和视野数据诊断青光眼的新方法。
在单一青光眼中心,确定了 1499 只青光眼疑似眼和 895 只青光眼眼的数据。每只眼都接受了海德堡视网膜断层扫描仪(HRT)成像和标准自动视野计检查。通过三个步骤定义了一种将这两种测试结合起来的新测量方法,即结构功能指数(SFI):1)计算每个视野点异常的概率;2)计算 HRT 视盘 6 个扇形区异常的概率;3)将这些概率与视野点和视盘区通过神经节细胞解剖结构的概率结合起来。使用受试者工作特征(ROC)分析比较 SFI 与 HRT 和视野。
SFI 产生的 ROC 曲线下面积(0.78)与视野平均偏差(0.78)和模式标准偏差(0.80)相似,大于 HRT 边缘面积的归一化测量值(0.66)。各种测试分类为青光眼的病例明显不重叠。根据轻度疾病人群中测试值的分布,SFI 可能更能对该组进行分层,同时仍能清楚地识别出严重疾病的患者。
SFI 通过结合视神经结构和功能反映了传统的青光眼临床诊断。通过这样做,它确定了与单独进行视野测试或视神经头成像不同的患者子集。对前瞻性数据的分析将使我们能够确定结构和功能的综合指数是否可以为青光眼诊断提供改进的标准。