Shin Kyung Hyun, Chang Ho-Guen, Rhee Nam Kyou, Lim Kwahn Sue
Department of Orthopaedic Surgery, Shin Hospital, Suwon, Korea.
Asian Spine J. 2011 Mar;5(1):1-9. doi: 10.4184/asj.2011.5.1.1. Epub 2011 Mar 2.
A retrospective study.
To determine the feasibility and effectiveness of revisional percutaneous full endoscopic discectomy for recurrent herniation after conventional open disc surgery. OVERVIEW OF THE LITERATURE: Repeated open discectomy with or without fusion has been the most common procedure for recurrent lumbar disc herniation. Percutaneous endoscopic lumbar discectomy for recurrent herniation has been thought of as an impossible procedure. Despite good results with open revisional surgery, major problems may be caused by injuries to the posterior stabilized structures. Our team did revisional full endoscopic lumbar disc surgery on the basis of our experience doing primary full endoscopic disc surgery.
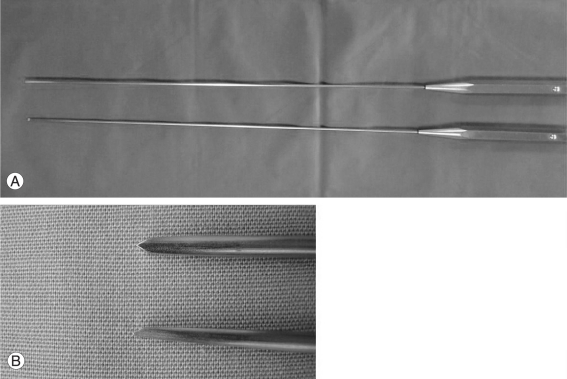
Between February 2004 and August 2009 a total of 41 patients in our hospital underwent revisional percutaneous endoscopic lumbar discectomy using a YESS endoscopic system and a micro-osteotome (designed by the authors). Indications for surgery were recurrent disc herniation following conventional open discectomy; with compression of the nerve root revealed by Gadolinium-enhanced magnetic resonance imaging; corresponding radiating pain which was not alleviated after conservative management over 6 weeks. Patients with severe neurologic deficits and isolated back pain were excluded.
The mean follow-up period was 16 months (range, 13 to 42 months). The visual analog scale for pain in the leg and back showed significant post-treatment improvement (p < 0.001). Based on a modified version of MacNab's criteria, 90.2% showed excellent or good outcomes. There was no measurable blood loss. There were two cases of recurrence of and four cases with complications.
Percutaneous full-endoscopic revisional disc surgery without additional structural damage is feasible and effective in terms of there being less chance of fusion and bleeding. This technique can be an alternative to conventional repeated discectomy.
一项回顾性研究。
确定经皮全内镜翻修椎间盘切除术治疗传统开放性椎间盘手术后复发性椎间盘突出症的可行性和有效性。
有或没有融合的重复开放性椎间盘切除术一直是复发性腰椎间盘突出症最常见的手术方式。经皮内镜下腰椎间盘切除术治疗复发性椎间盘突出症一直被认为是不可能的手术。尽管开放性翻修手术效果良好,但对后方稳定结构的损伤可能会导致严重问题。我们的团队在进行初次全内镜椎间盘手术的经验基础上开展了翻修性全内镜腰椎间盘手术。
2004年2月至2009年8月期间,我院共有41例患者接受了使用YESS内镜系统和微型骨刀(由作者设计)的经皮内镜下腰椎间盘翻修切除术。手术适应症为传统开放性椎间盘切除术后复发性椎间盘突出症;钆增强磁共振成像显示神经根受压;经6周以上保守治疗后相应的放射性疼痛未缓解。排除有严重神经功能缺损和单纯背痛的患者。
平均随访期为16个月(范围13至42个月)。腿部和背部疼痛的视觉模拟量表显示治疗后有显著改善(p < 0.001)。根据改良版MacNab标准,90.2%的患者显示出优良结果。术中无明显失血。有2例复发和4例出现并发症。
经皮全内镜翻修椎间盘手术无额外结构损伤,在减少融合和出血可能性方面是可行且有效的。该技术可作为传统重复椎间盘切除术的替代方法。