College for Management in Healthcare and Forum Managed Care (FMC), Freiburgstrasse 41, CH-3010 Bern, Switzerland.
Int J Integr Care. 2011 Jan;11 Spec Ed(Special 10th Anniversary Edition):e010. Epub 2011 Mar 14.
The Swiss health care system is characterized by its decentralized structure and high degree of local autonomy. Ambulatory care is provided by physicians working mainly independently in individual private practices. However, a growing part of primary care is provided by networks of physicians and health maintenance organizations (HMOs) acting on the principles of gatekeeping.
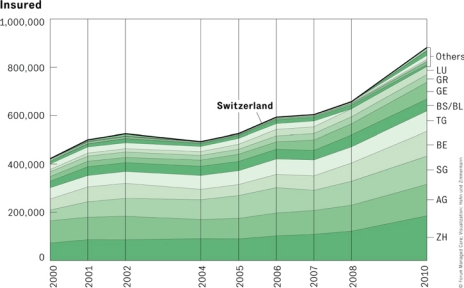
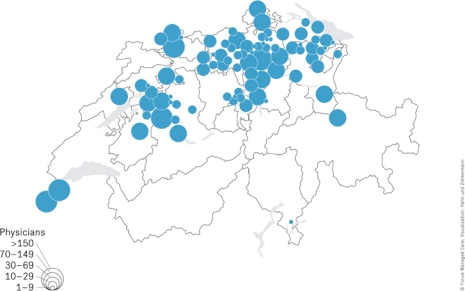
The share of insured choosing an alternative (managed care) type of basic health insurance and therefore restrict their choice of doctors in return for lower premiums increased continuously since 1990. To date, an average of one out of eight insured person in Switzerland, and one out of three in the regions in north-eastern Switzerland, opted for the provision of care by general practitioners in one of the 86 physician networks or HMOs. About 50% of all general practitioners and more than 400 other specialists have joined a physician networks. Seventy-three of the 86 networks (84%) have contracts with the healthcare insurance companies in which they agree to assume budgetary co-responsibility, i.e., to adhere to set cost targets for particular groups of patients. Within and outside the physician networks, at regional and/or cantonal levels, several initiatives targeting chronic diseases have been developed, such as clinical pathways for heart failure and breast cancer patients or chronic disease management programs for patients with diabetes.
Swiss physician networks and HMOs were all established solely by initiatives of physicians and health insurance companies on the sole basis of a healthcare legislation (Swiss Health Insurance Law, KVG) which allows for such initiatives and developments. The relevance of these developments towards more integration of healthcare as well as their implications for the future are discussed.
瑞士的医疗保健系统以其分散的结构和高度的地方自治为特点。门诊护理由主要在个体私人诊所独立工作的医生提供。然而,越来越多的初级保健工作是由按照守门人原则运作的医生网络和健康维护组织(HMO)提供的。
自 1990 年以来,选择替代(管理式医疗)类型基本健康保险并因此限制其选择医生以换取较低保费的参保人数不断增加。迄今为止,瑞士平均每八名参保人中就有一人,在瑞士东北部地区每三名参保人中就有一人选择在 86 个医生网络或 HMO 中的一个提供医生护理。大约 50%的全科医生和 400 多名其他专科医生已经加入了医生网络。86 个网络中的 73 个(84%)与医疗保险公司签订了合同,同意承担预算共同责任,即遵守特定患者群体的设定成本目标。在医生网络内部和外部,在区域和/或州一级,已经制定了针对慢性病的多项倡议,例如心力衰竭和乳腺癌患者的临床路径或糖尿病患者的慢性病管理计划。
瑞士的医生网络和 HMO 都是由医生和健康保险公司单独根据允许此类倡议和发展的医疗保健立法(瑞士健康保险法,KVG)的唯一基础建立的。讨论了这些发展对医疗保健更整合的相关性及其对未来的影响。