Department of Surgery, The Johns Hopkins University School of Medicine, Baltimore, MD 21287, USA.
J Gastrointest Surg. 2011 Nov;15(11):2089-97. doi: 10.1007/s11605-011-1614-7. Epub 2011 Jul 2.
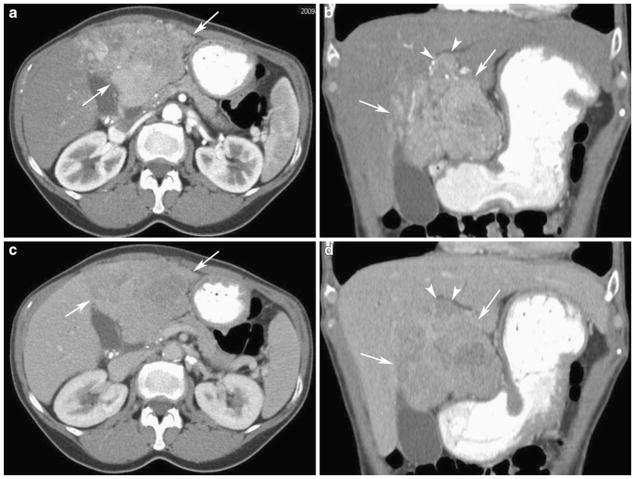
Hepatocellular carcinoma (HCC) is a leading cause of cancer-related death worldwide. It is traditionally difficult to cure, especially when discovered at later stages, making early diagnosis and intervention of paramount importance. HCC typically arises in the background of chronic liver disease and can have various morphologic appearances. One of the most difficult of these to recognize on early surveillance imaging is the infiltrative subtype, which can account for up to 13% of all HCC cases, and may be more closely associated with background hepatitis B infection.
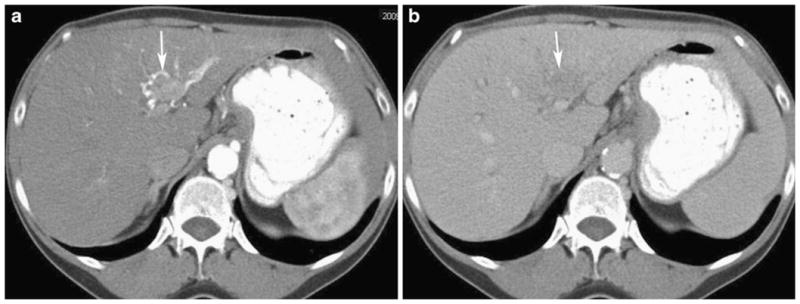
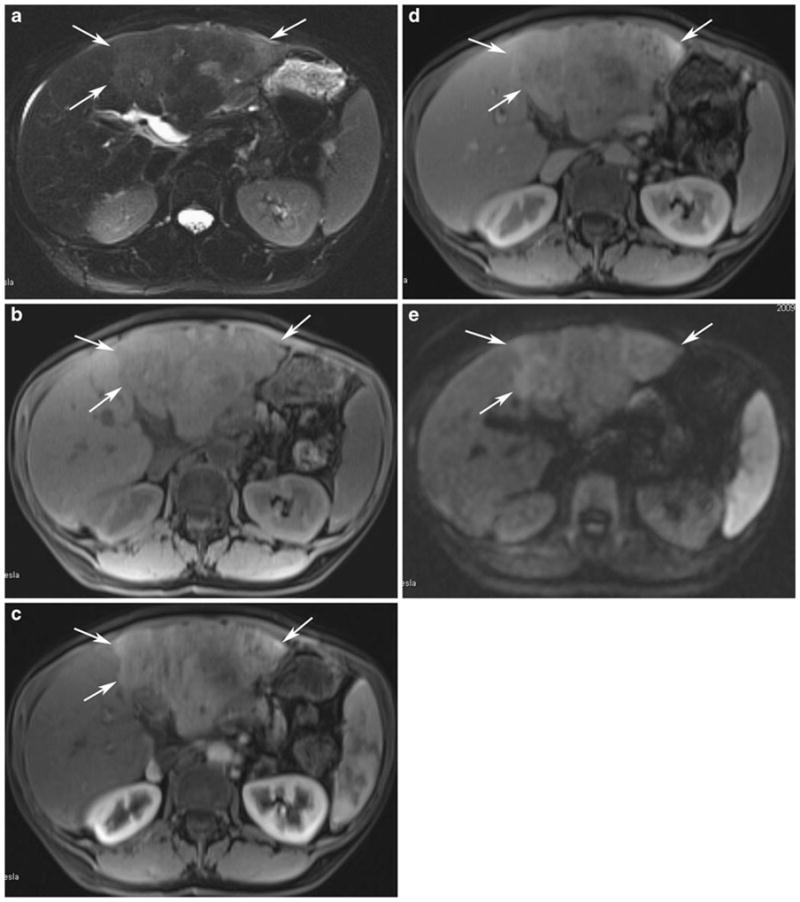
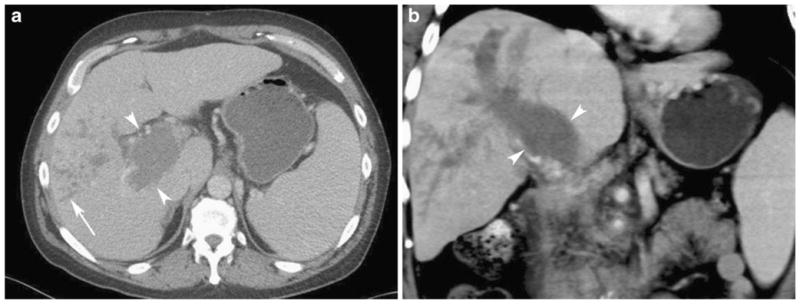
Certain imaging characteristics can provide vital clues, including differing signal intensity on the T1 and T2 sequences of magnetic resonance imaging (MRI) and the presence/appearance of portal vein thrombus. Owing to the diffuse and infiltrating properties of this tumor, surgical resection and transplantation are rarely if ever viable therapeutic options. Other forms of liver-directed therapy have been attempted with limited success, having minimal efficacy and high morbidity. To date, there is no data available to determine if the various HCC subtypes respond to systemic therapy differently, so this may be the most reasonable approach. Left untreated, observed patients commonly progress to hepatic failure fairly rapidly.
Infiltrative HCC can be extremely subtle, and therefore difficult to detect, especially in the background of cirrhosis. Providers caring for patients with hepatitis, chronic liver disease, and cirrhosis must be extremely vigilant in the evaluation of surveillance imaging in order to potentially discover this HCC subtype as early as possible and initiate a multidisciplinary treatment plan.
肝细胞癌(HCC)是全球癌症相关死亡的主要原因。传统上,这种疾病很难治愈,尤其是在晚期发现时,因此早期诊断和干预至关重要。HCC 通常在慢性肝病的背景下发生,其形态表现多样。其中最难在早期监测影像中识别的是浸润性亚型,它可能占所有 HCC 病例的 13%,并且可能与乙型肝炎感染的背景更为密切相关。
某些影像学特征可以提供重要线索,包括磁共振成像(MRI)T1 和 T2 序列上的信号强度差异,以及门静脉血栓的存在/表现。由于肿瘤具有弥漫性和浸润性,手术切除和移植很少是可行的治疗选择。其他形式的肝定向治疗也有尝试,但效果有限,发病率高。迄今为止,尚无数据可确定不同 HCC 亚型对系统治疗的反应是否不同,因此这可能是最合理的方法。未接受治疗的患者通常会很快进展为肝衰竭。
浸润性 HCC 可能非常微妙,因此很难检测到,尤其是在肝硬化的背景下。照顾肝炎、慢性肝病和肝硬化患者的医务人员必须在评估监测影像时保持高度警惕,以便尽早发现这种 HCC 亚型,并启动多学科治疗计划。