International Centre for Circulatory Health, Imperial College London, 59 North Wharf Road, London, UK.
Eur Heart J. 2012 Feb;33(4):486-94. doi: 10.1093/eurheartj/ehr262. Epub 2011 Jul 28.
We tested whether on-statin C-reactive protein is associated with cardiovascular (CV) outcome in the Anglo-Scandinavian Cardiac Outcomes Trial (ASCOT).
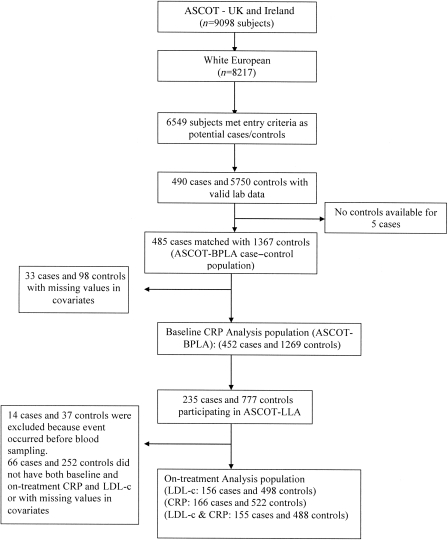
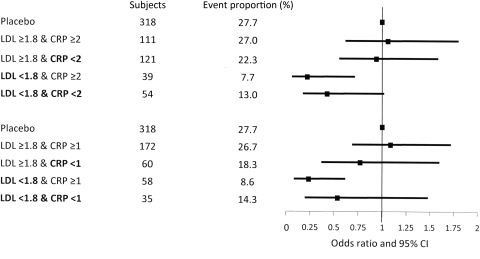
ASCOT randomized a subset of 4853 patients with total cholesterol ≤6.5 mmol/L (250 mg/dL) to atorvastatin or placebo. In a case-control study during 5.5-year follow-up, 485 CV cases were age- and sex-matched with 1367 controls. Baseline LDL-cholesterol (LDL-c) and log-transformed C-reactive protein predicted CV events [odds ratio (OR) per 1 standard deviation (SD) 1.31 (95% confidence interval {CI}: 1.10, 1.56), P = 0.002 and OR 1.19 (1.05, 1.34), P = 0.006, respectively]. Including baseline C-reactive protein into a Framingham risk model very modestly improved risk prediction. Baseline C-reactive protein did not indicate the magnitude of the atorvastatin effect on CV outcome (P = 0.54). At 6 months, atorvastatin reduced median LDL-c by 40.3% and median C-reactive protein by 27.4%. In those randomized to atorvastatin, lower on-treatment LDL-c at 6 months was associated with a significant reduction in subsequent CV events [OR 0.41 (0.22, 0.75), P = 0.004] comparing those above and below the median (2.1 mmol/L). In contrast, C-reactive protein below the median (1.83 mg/L) compared with C-reactive protein above the median was not associated with a significant reduction in CV events [OR 0.86 (0.49, 1.51), P = 0.60]. Consequently, addition of on-treatment C-reactive protein to LDL-c did not improve prediction of statin efficacy.
Among these hypertensive patients selected on the basis of traditional CV risk factors, C-reactive protein did not usefully improve the prediction of CV events and, critically, reduction in C-reactive protein associated with statin therapy was not a predictor of CV outcome alone or in combination with LDL-c.
我们旨在检测在盎格鲁-斯堪的纳维亚心脏终点试验(ASCOT)中,他汀类药物治疗患者的 C 反应蛋白(CRP)与心血管(CV)结局的相关性。
ASCOT 试验将胆固醇水平≤6.5mmol/L(250mg/dL)的患者随机分为阿托伐他汀组或安慰剂组。在 5.5 年的随访期间,采用病例对照研究,对 4853 例患者中的 485 例 CV 病例和 1367 例对照进行了年龄和性别匹配。基线 LDL-胆固醇(LDL-c)和 CRP 的自然对数值(lnCRP)均与 CV 事件相关[每增加一个标准差(SD)的比值比(OR)分别为 1.31(95%可信区间{CI}:1.10,1.56),P=0.002 和 1.19(1.05,1.34),P=0.006]。将基线 CRP 纳入 Framingham 风险模型后,可略微提高风险预测的准确性。基线 CRP 并不能反映阿托伐他汀对 CV 结局的影响程度(P=0.54)。阿托伐他汀治疗 6 个月后,可降低 LDL-c 中位数 40.3%和 CRP 中位数 27.4%。在接受阿托伐他汀治疗的患者中,6 个月时 LDL-c 水平越低,随后发生 CV 事件的风险显著降低[比值比(OR)0.41(0.22,0.75),P=0.004],与中位数以上和以下的患者相比。相比之下,与 CRP 中位数以上的患者相比,CRP 中位数以下的患者的 CV 事件发生率并未显著降低[OR 0.86(0.49,1.51),P=0.60]。因此,将治疗中的 CRP 与 LDL-c 联合应用并未改善他汀类药物疗效的预测。
在基于传统 CV 危险因素选择的高血压患者中,CRP 不能有效地预测 CV 事件,并且 CRP 降低与他汀类药物治疗相关,这不能单独预测 CV 结局,也不能与 LDL-c 联合预测。