Mathematical, Computational, and Modeling Sciences Center, Arizona State University, Tempe, AZ, USA.
BMC Infect Dis. 2011 Aug 1;11:207. doi: 10.1186/1471-2334-11-207.
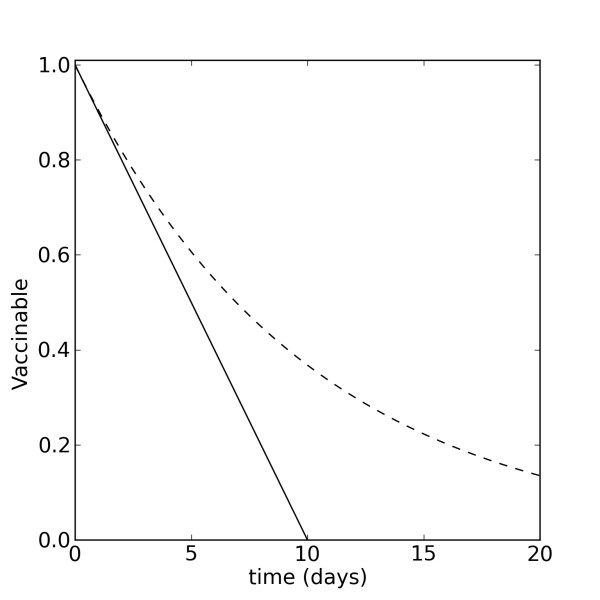
Influenza viruses are a major cause of morbidity and mortality worldwide. Vaccination remains a powerful tool for preventing or mitigating influenza outbreaks. Yet, vaccine supplies and daily administration capacities are limited, even in developed countries. Understanding how such constraints can alter the mitigating effects of vaccination is a crucial part of influenza preparedness plans. Mathematical models provide tools for government and medical officials to assess the impact of different vaccination strategies and plan accordingly. However, many existing models of vaccination employ several questionable assumptions, including a rate of vaccination proportional to the population at each point in time.
We present a SIR-like model that explicitly takes into account vaccine supply and the number of vaccines administered per day and places data-informed limits on these parameters. We refer to this as the non-proportional model of vaccination and compare it to the proportional scheme typically found in the literature.
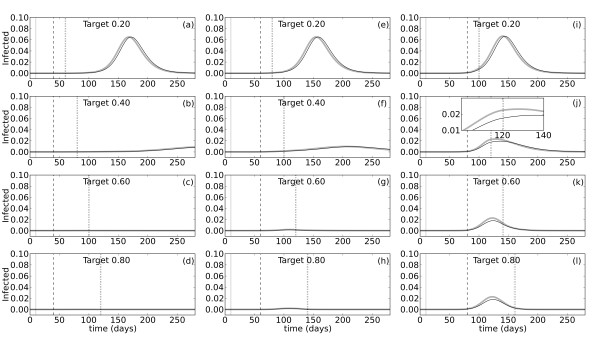
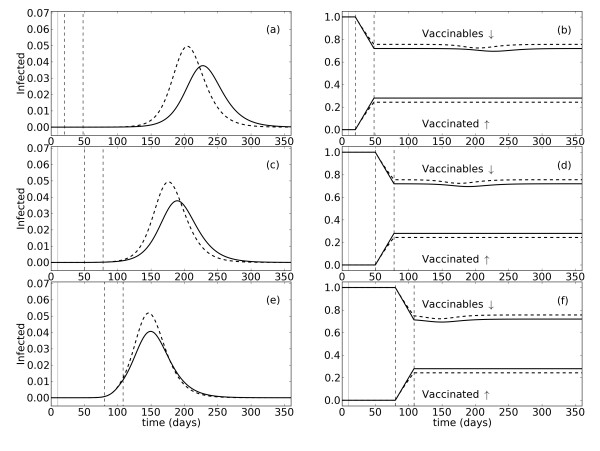
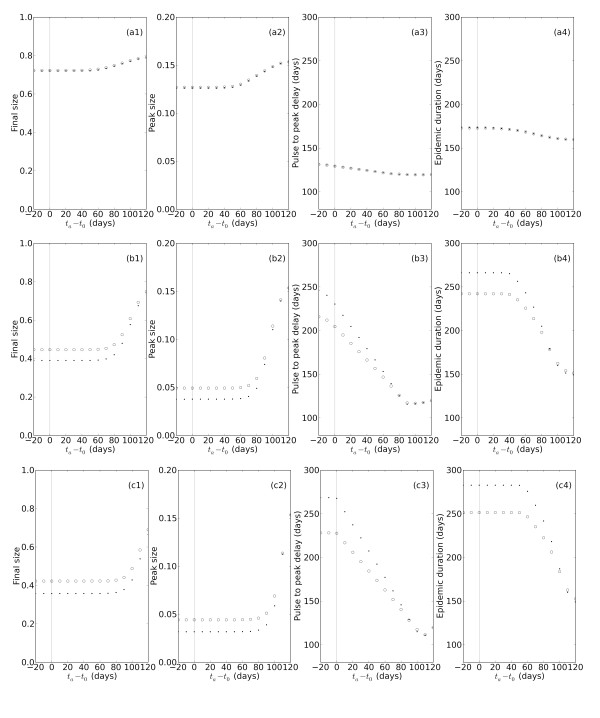
The proportional and non-proportional models behave similarly for a few different vaccination scenarios. However, there are parameter regimes involving the vaccination campaign duration and daily supply limit for which the non-proportional model predicts smaller epidemics that peak later, but may last longer, than those of the proportional model. We also use the non-proportional model to predict the mitigating effects of variably timed vaccination campaigns for different levels of vaccination coverage, using specific constraints on daily administration capacity.
The non-proportional model of vaccination is a theoretical improvement that provides more accurate predictions of the mitigating effects of vaccination on influenza outbreaks than the proportional model. In addition, parameters such as vaccine supply and daily administration limit can be easily adjusted to simulate conditions in developed and developing nations with a wide variety of financial and medical resources. Finally, the model can be used by government and medical officials to create customized pandemic preparedness plans based on the supply and administration constraints of specific communities.
流感病毒是全球发病率和死亡率的主要原因。疫苗接种仍然是预防或减轻流感爆发的有力工具。然而,即使在发达国家,疫苗供应和日常管理能力也有限。了解这些限制如何改变疫苗接种的缓解效果是流感防范计划的重要组成部分。数学模型为政府和医疗官员提供了评估不同疫苗接种策略影响并相应计划的工具。然而,许多现有的疫苗接种模型采用了几个有问题的假设,包括疫苗接种率与每个时间点的人口成正比。
我们提出了一个类似于 SIR 的模型,该模型明确考虑了疫苗供应和每天接种的疫苗数量,并对这些参数进行了数据驱动的限制。我们将其称为非比例疫苗接种模型,并将其与文献中通常发现的比例方案进行比较。
对于几种不同的疫苗接种情况,比例和非比例模型的行为相似。然而,在涉及疫苗接种活动持续时间和每日供应限制的参数范围内,非比例模型预测的疫情较小,峰值较晚,但可能持续时间更长,而比例模型则预测的疫情较大,峰值较早。我们还使用非比例模型来预测不同疫苗接种覆盖率水平下不同时间安排的疫苗接种活动的缓解效果,同时使用每日管理能力的具体限制。
非比例疫苗接种模型是一种理论上的改进,它比比例模型更准确地预测了疫苗接种对流感爆发的缓解效果。此外,疫苗供应和每日管理限制等参数可以轻松调整,以模拟具有各种财务和医疗资源的发达国家和发展中国家的情况。最后,该模型可由政府和医疗官员使用,根据特定社区的供应和管理限制制定定制的大流行性流感防范计划。