Department of Critical Care Medicine, Hospital for Sick Children, 555 University Avenue, Toronto, ON M5G 1X8, Canada.
Crit Care. 2011 Aug 3;15(4):R184. doi: 10.1186/cc10337.
The timely provision of critical care to hospitalised patients at risk for cardiopulmonary arrest is contingent upon identification and referral by frontline providers. Current approaches require improvement. In a single-centre study, we developed the Bedside Paediatric Early Warning System (Bedside PEWS) score to identify patients at risk. The objective of this study was to validate the Bedside PEWS score in a large patient population at multiple hospitals.
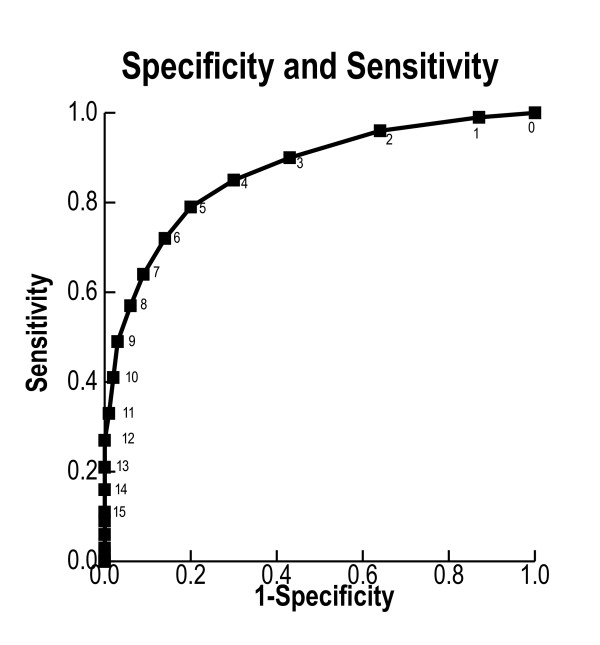
We performed an international, multicentre, case-control study of children admitted to hospital inpatient units with no limitations on care. Case patients had experienced a clinical deterioration event involving either an immediate call to a resuscitation team or urgent admission to a paediatric intensive care unit. Control patients had no events. The scores ranged from 0 to 26 and were assessed in the 24 hours prior to the clinical deterioration event. Score performance was assessed using the area under the receiver operating characteristic (AUCROC) curve by comparison with the retrospective rating of nurses and the temporal progression of scores in case patients.
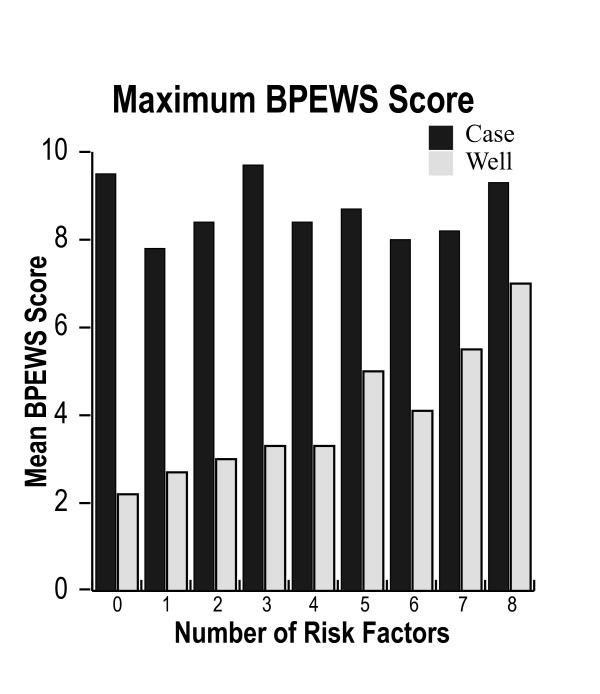
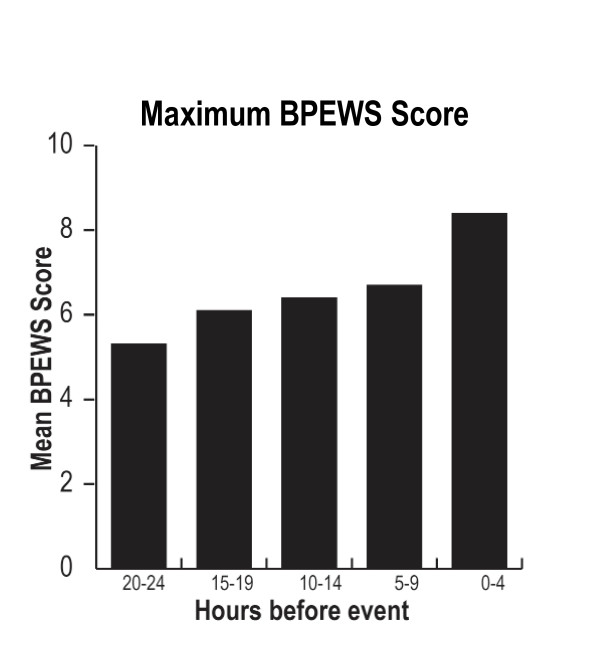
A total of 2,074 patients were evaluated at 4 participating hospitals. The median (interquartile range) maximum Bedside PEWS scores for the 12 hours ending 1 hour before the clinical deterioration event were 8 (5 to 12) in case patients and 2 (1 to 4) in control patients (P < 0.0001). The AUCROC curve (95% confidence interval) was 0.87 (0.85 to 0.89). In case patients, mean scores were 5.3 at 20 to 24 hours and 8.4 at 0 to 4 hours before the event (P < 0.0001). The AUCROC curve (95% CI) of the retrospective nurse ratings was 0.83 (0.81 to 0.86). This was significantly lower than that of the Bedside PEWS score (P < 0.0001).
The Bedside PEWS score identified children at risk for cardiopulmonary arrest. Scores were elevated and continued to increase in the 24 hours before the clinical deterioration event. Prospective clinical evaluation is needed to determine whether this score will improve the quality of care and patient outcomes.
及时为有发生心肺骤停风险的住院患者提供重症监护取决于一线医护人员的识别和转介。目前的方法需要改进。在一项单中心研究中,我们开发了床边儿科早期预警系统(Bedside PEWS)评分来识别有风险的患者。本研究的目的是在多家医院的大量患者群体中验证床边 PEWS 评分。
我们进行了一项国际性的多中心病例对照研究,纳入了无任何医疗限制的住院病房患儿。病例组患者经历了涉及到紧急呼叫复苏团队或紧急转入儿科重症监护病房的临床恶化事件。对照组患者无此类事件。评分范围为 0 至 26 分,在临床恶化事件发生前的 24 小时内进行评估。通过与护士回顾性评分和病例组评分的时间进展比较,使用接受者操作特征(ROC)曲线下面积(AUCROC)评估评分表现。
4 家参与医院共评估了 2074 例患者。在距临床恶化事件发生前 1 小时结束的 12 小时内,病例组最大床边 PEWS 评分中位数(四分位距)为 8(5 至 12),对照组为 2(1 至 4)(P<0.0001)。AUCROC 曲线(95%置信区间)为 0.87(0.85 至 0.89)。在病例组中,平均评分在 20 至 24 小时为 5.3,在事件发生前 0 至 4 小时为 8.4(P<0.0001)。护士回顾性评分的 AUCROC 曲线(95%CI)为 0.83(0.81 至 0.86)。这明显低于床边 PEWS 评分(P<0.0001)。
床边 PEWS 评分可识别有发生心肺骤停风险的儿童。评分在临床恶化事件发生前 24 小时升高且持续升高。需要前瞻性临床评估以确定该评分是否会改善护理质量和患者结局。