Department of Medicine, University of Chicago, Chicago, Illinois 60637, USA.
Clin Infect Dis. 2011 Sep;53(5):440-7. doi: 10.1093/cid/cir404.
Treatment guidelines recommend stopping all implicated antibiotics at the onset of Clostridium difficile infection (CDI), but many individuals have persistent or new infections necessitating the use of concomitant antibiotics (CAs). We used data from 2 phase 3 trials to study effects of CAs on response to fidaxomicin or vancomycin.
Subjects with CDI were treated for 10 days with fidaxomicin 200 mg every 12 hours or vancomycin 125 mg every 6 hours, assessed for resolution of symptoms, and followed up for an additional 4 weeks for evidence of recurrence. Rates of cure, recurrence, and global cure (cure without recurrence) were determined for subgroups of subjects defined by CA use and treatment group.
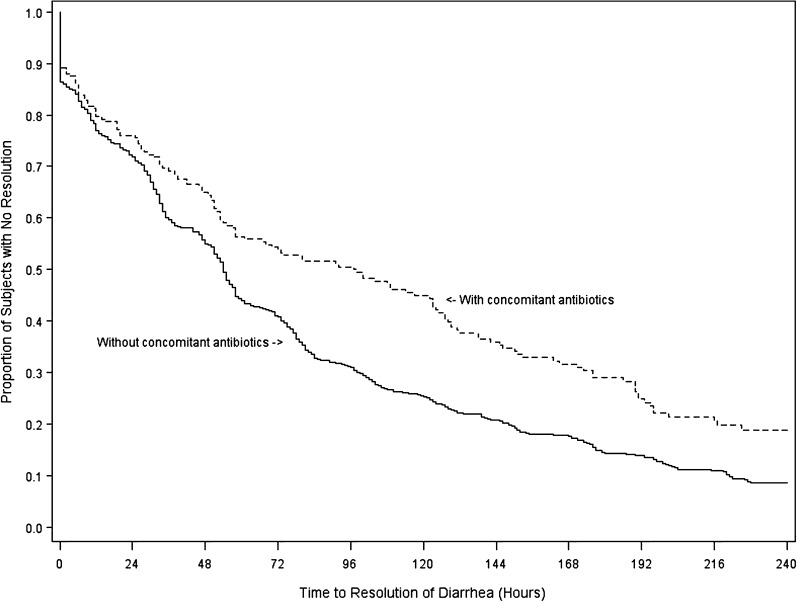
CAs were prescribed for 27.5% of subjects during study participation. The use of CAs concurrent with CDI treatment was associated with a lower cure rate (84.4% vs 92.6%; P < .001) and an extended time to resolution of diarrhea (97 vs 54 hours; P < .001). CA use during the follow-up was associated with more recurrences (24.8% vs 17.7%; not significant), and CA administration at any time was associated with a lower global cure rate (65.8% vs 74.7%; P = .005). When subjects received CAs concurrent with CDI treatment, the cure rate was 90.0% for fidaxomicin and 79.4% for vancomycin (P = .04). In subjects receiving CAs during treatment and/or follow-up, treatment with fidaxomicin compared with vancomycin was associated with 12.3% fewer recurrences (16.9% vs 29.2%; P = .048).
Treatment with CAs compromised initial response to CDI therapy and durability of response. Fidaxomicin was significantly more effective than vancomycin in achieving clinical cure in the presence of CA therapy and in preventing recurrence regardless of CA use.
治疗指南建议在艰难梭菌感染(CDI)发作时停止所有可疑抗生素,但许多患者仍存在持续性或新发感染,需要使用合并抗生素(CA)。我们使用两项 3 期试验的数据来研究 CA 对 fidaxomicin 或万古霉素应答的影响。
CDI 患者接受 fidaxomicin 200mg 每 12 小时或万古霉素 125mg 每 6 小时治疗 10 天,评估症状缓解情况,并在后续 4 周内观察复发证据。根据 CA 使用和治疗组,确定治疗亚组患者的治愈率、复发率和总体治愈率(无复发治愈率)。
研究期间,27.5%的患者处方 CA。在 CDI 治疗期间同时使用 CA 与较低的治愈率(84.4% vs 92.6%;P<0.001)和腹泻缓解时间延长(97 小时 vs 54 小时;P<0.001)相关。在随访期间使用 CA 与更多复发(24.8% vs 17.7%;无显著差异)相关,任何时间使用 CA 与较低的总体治愈率(65.8% vs 74.7%;P=0.005)相关。当患者在接受 CDI 治疗的同时接受 CA 治疗时,fidaxomicin 的治愈率为 90.0%,万古霉素为 79.4%(P=0.04)。在接受治疗和/或随访期间使用 CA 的患者中,与万古霉素相比,fidaxomicin 治疗与 12.3%的复发率降低相关(16.9% vs 29.2%;P=0.048)。
CA 治疗降低了对 CDI 治疗的初始应答和应答的持久性。在 CA 治疗存在的情况下,fidaxomicin 与万古霉素相比,在实现临床治愈方面显著更有效,并能预防复发,无论 CA 是否使用。