General Practice Research Database, Medicines and Healthcare products Regulatory Agency, 151 Buckingham Palace Road, London SW1W 9SZ, UK.
Eur Heart J. 2011 Oct;32(19):2376-86. doi: 10.1093/eurheartj/ehr340. Epub 2011 Aug 29.
Adherence to evidence-based treatments and its consequences after acute myocardial infarction (MI) are poorly defined. We examined the extent to which clopidogrel treatment initiated in hospital is continued in primary care; the factors predictive of clopidogrel discontinuation and the hazard of death or recurrent MI.
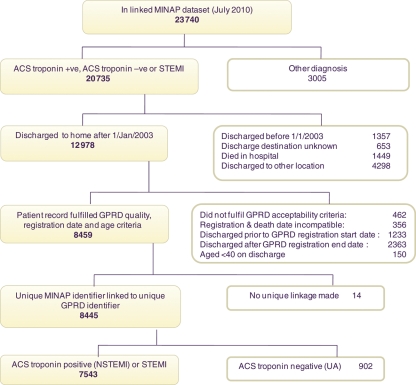
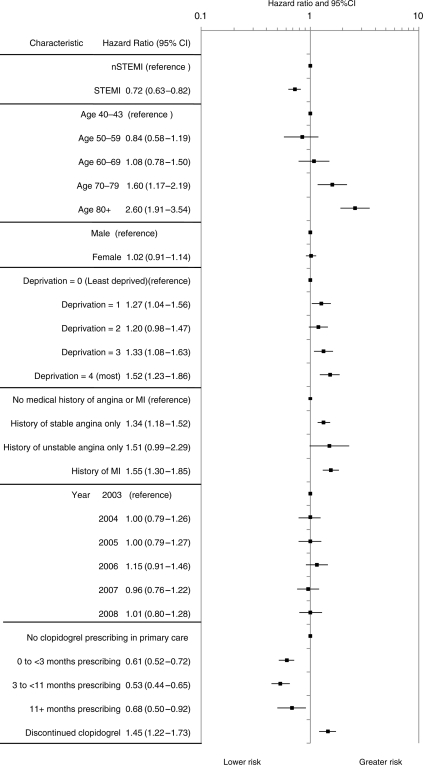
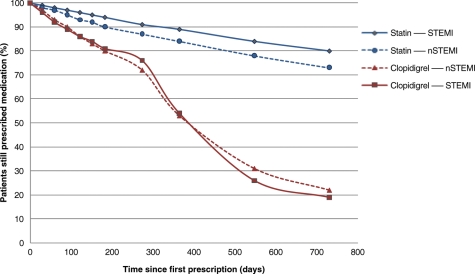
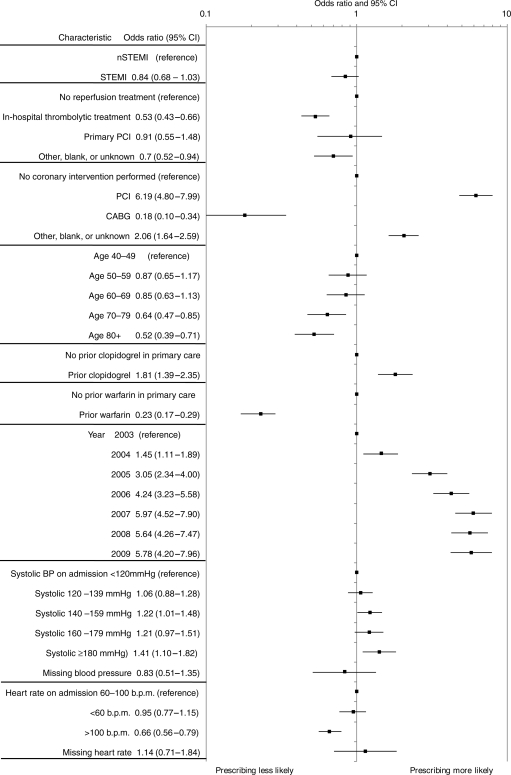
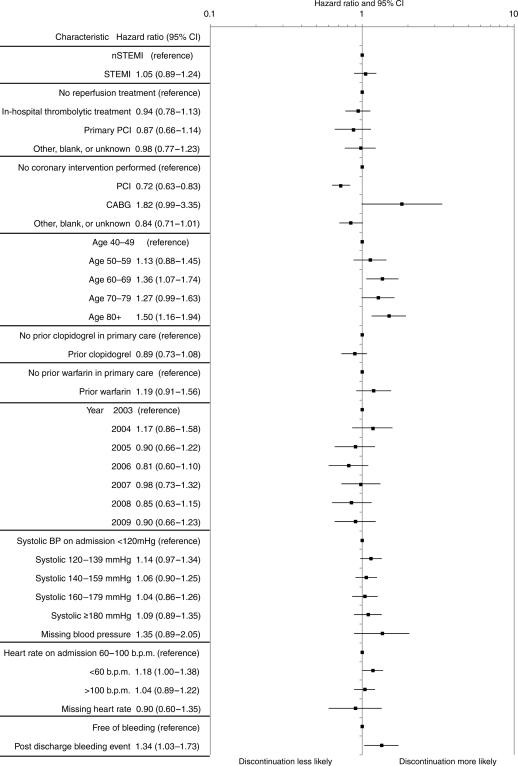
We linked the Myocardial Ischaemia National Audit Project registry and the General Practice Research Database to examine adherence to clopidogrel in primary care among patients discharged from hospital after MI (2003-2009). Hospital Episode Statistics and national mortality data were linked, documenting all-cause mortality and non-fatal MI. Of the 7543 linked patients, 4650 were prescribed clopidogrel in primary care within 3 months of discharge. The adjusted odds of still being prescribed clopidogrel at 12 months were similar following non-ST-elevation myocardial infarction (NSTEMI) 53% (95% CI, 51-55) and ST-elevation myocardial infarction (STEMI) 54% (95% CI, 52-56), but contrast with statins: NSTEMI 84% (95% CI, 82-85) and STEMI 89% (95% CI, 87-90). Discontinuation within 12 months was more frequent in older patients [>80 vs. 40-49 years, adjusted hazard ratio (HR) 1.50 (95% CI, 1.15-1.94)] and with bleeding events [HR 1.34 (95% CI, 1.03-1.73)]. 18.15 patients per 100 person-years (95% CI, 16.83-19.58) died or experienced non-fatal MI in the first year following discharge. In patients who discontinued clopidogrel within 12 months, the adjusted HR for death or non-fatal MI was 1.45 (95% CI, 1.22-1.73) compared with untreated patients, and 2.62 (95% CI, 2.17-3.17) compared with patients persisting with clopidogrel treatment.
This is the first study to use linked registries to determine persistence of clopidogrel treatment after MI in primary care. It demonstrates that discontinuation is common and associated with adverse outcomes.
急性心肌梗死(MI)后,基于证据的治疗方法的依从性及其后果尚不清楚。我们研究了在医院启动的氯吡格雷治疗在初级保健中的延续程度;预测氯吡格雷停药的因素以及死亡或复发性 MI 的危险。
我们将心肌缺血国家审计项目登记处和一般实践研究数据库联系起来,以检查 MI 出院后(2003-2009 年)患者在初级保健中对氯吡格雷的依从性。医院发病统计数据和国家死亡率数据被联系起来,记录所有原因的死亡率和非致命性 MI。在 7543 名被链接的患者中,有 4650 名在出院后 3 个月内在初级保健中开了氯吡格雷。非 ST 段抬高型心肌梗死(NSTEMI)53%(95%CI,51-55)和 ST 段抬高型心肌梗死(STEMI)54%(95%CI,52-56)后 12 个月仍在服用氯吡格雷的调整后的可能性相似,但与他汀类药物不同:NSTEMI 84%(95%CI,82-85)和 STEMI 89%(95%CI,87-90)。在 12 个月内停药的患者更常见于老年患者[>80 岁与 40-49 岁,调整后的危险比(HR)1.50(95%CI,1.15-1.94)]和有出血事件的患者[HR 1.34(95%CI,1.03-1.73)]。在出院后第一年,每 100 人年有 18.15 名患者(95%CI,16.83-19.58)死亡或发生非致命性 MI。在 12 个月内停止使用氯吡格雷的患者中,与未治疗患者相比,死亡或非致命性 MI 的调整 HR 为 1.45(95%CI,1.22-1.73),与继续氯吡格雷治疗的患者相比,为 2.62(95%CI,2.17-3.17)。
这是第一项使用链接登记处来确定 MI 后初级保健中氯吡格雷治疗持续时间的研究。它表明停药很常见,并且与不良后果有关。