Hull York Medical School, Hull, United Kingdom.
PLoS Med. 2011 Sep;8(9):e1001098. doi: 10.1371/journal.pmed.1001098. Epub 2011 Sep 27.
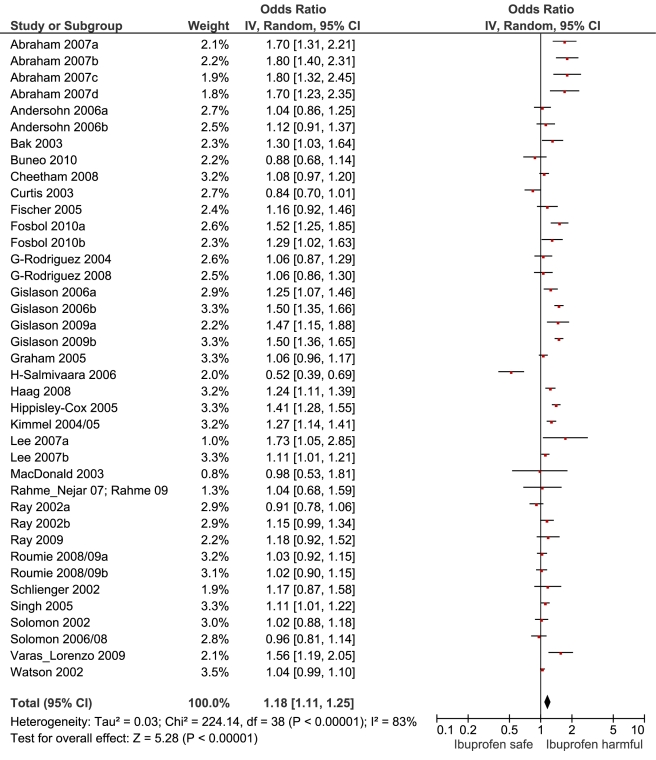
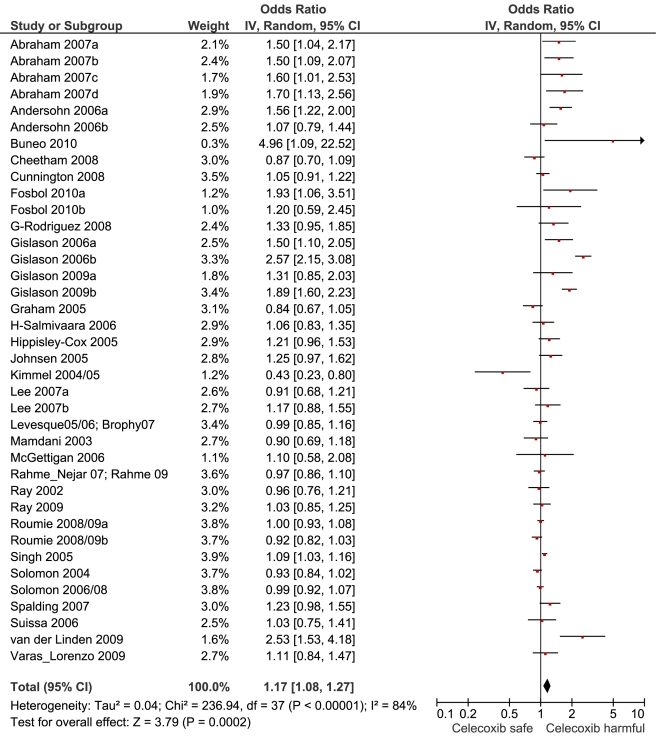
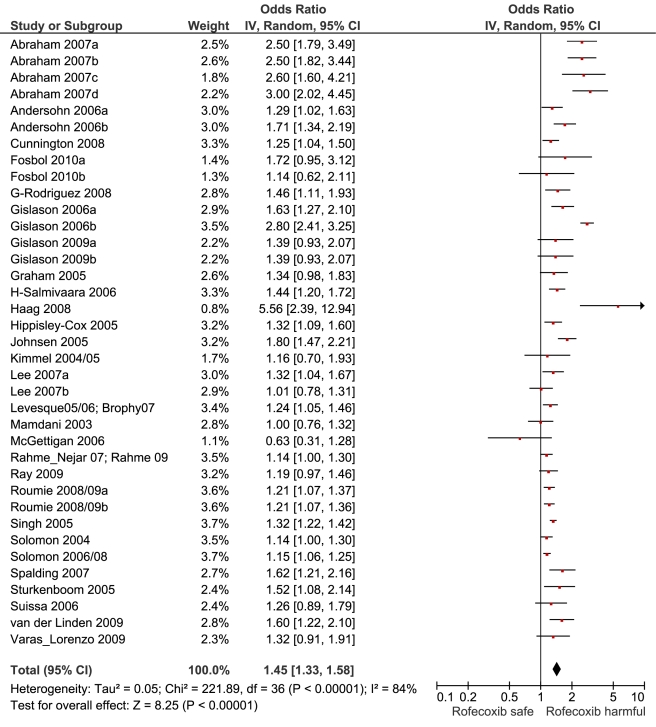
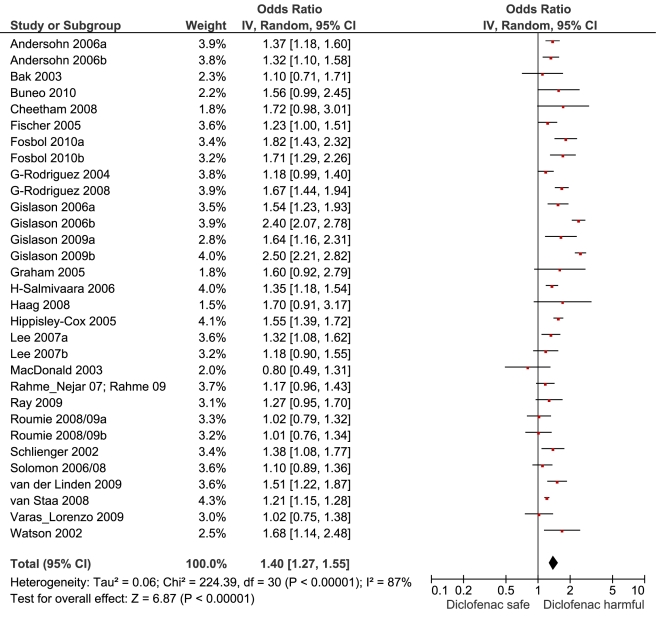
Randomised trials have highlighted the cardiovascular risks of non-steroidal anti-inflammatory drugs (NSAIDs) in high doses and sometimes atypical settings. Here, we provide estimates of the comparative risks with individual NSAIDs at typical doses in community settings.
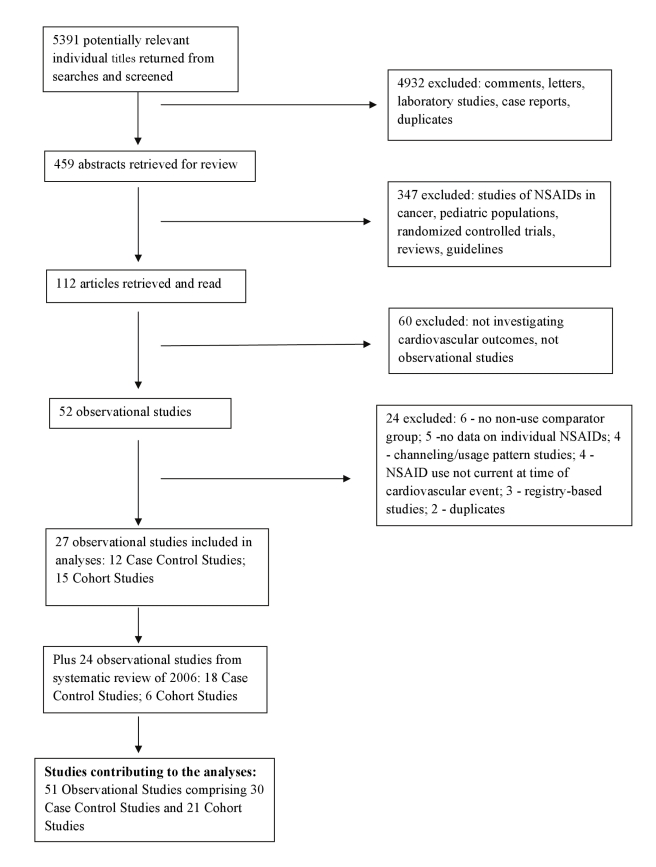
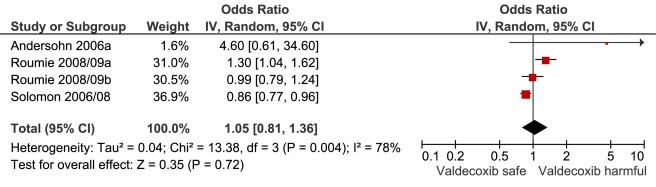
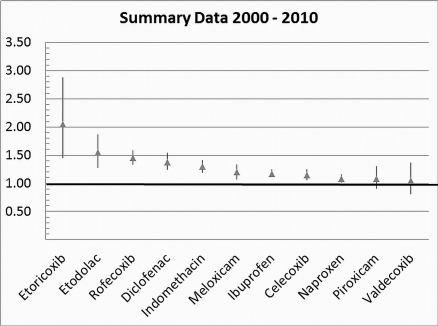
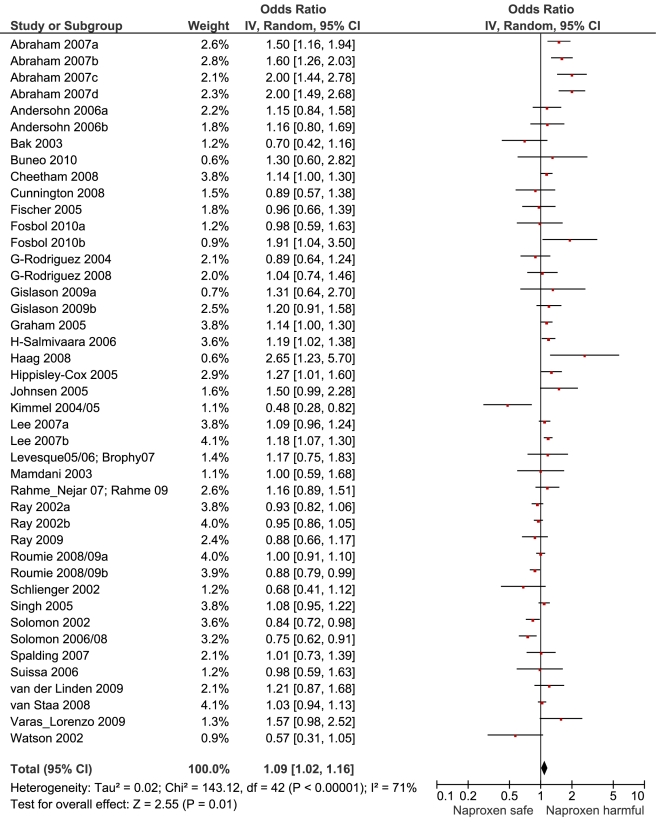
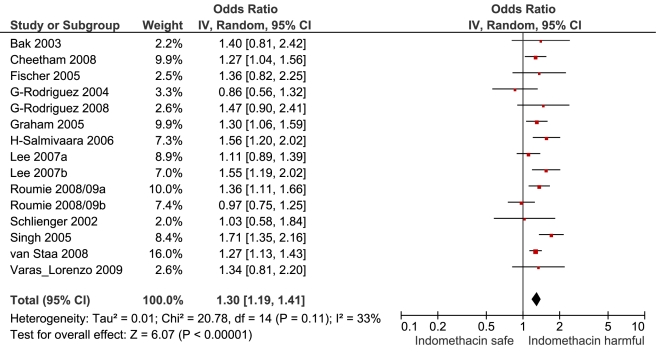
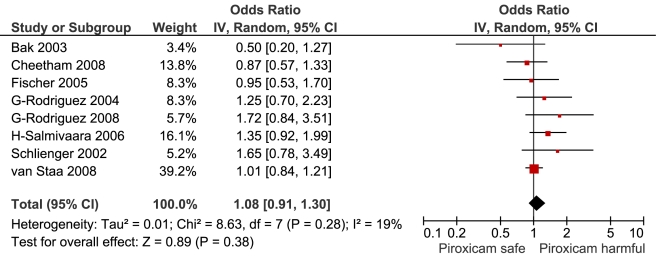
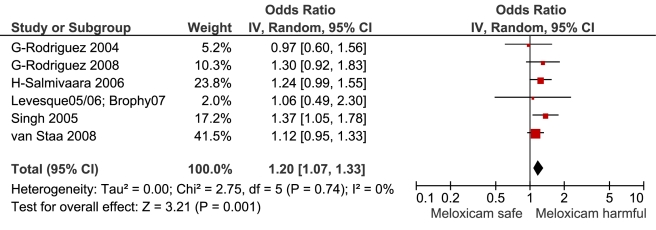
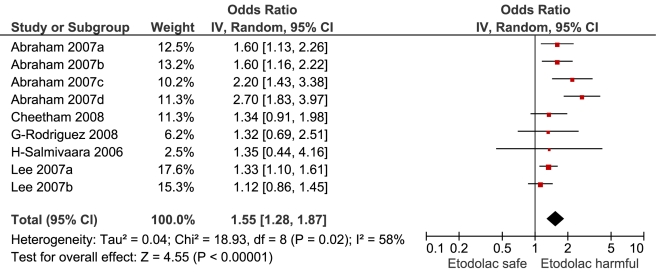
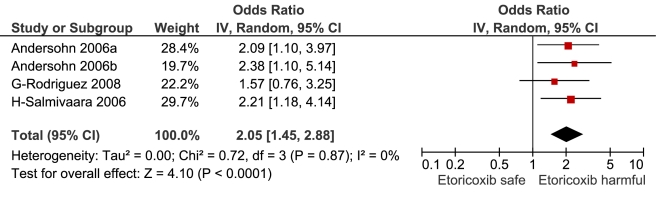
We performed a systematic review of community-based controlled observational studies. We conducted comprehensive literature searches, extracted adjusted relative risk (RR) estimates, and pooled the estimates for major cardiovascular events associated with use of individual NSAIDs, in different doses, and in populations with low and high background risks of cardiovascular events. We also compared individual drugs in pair-wise (within study) analyses, generating ratios of RRs (RRRs). Thirty case-control studies included 184,946 cardiovascular events, and 21 cohort studies described outcomes in >2.7 million exposed individuals. Of the extensively studied drugs (ten or more studies), the highest overall risks were seen with rofecoxib, 1.45 (95% CI 1.33, 1.59), and diclofenac, 1.40 (1.27, 1.55), and the lowest with ibuprofen, 1.18 (1.11, 1.25), and naproxen, 1.09 (1.02, 1.16). In a sub-set of studies, risk was elevated with low doses of rofecoxib, 1.37 (1.20, 1.57), celecoxib, 1.26 (1.09, 1.47), and diclofenac, 1.22 (1.12, 1.33), and rose in each case with higher doses. Ibuprofen risk was seen only with higher doses. Naproxen was risk-neutral at all doses. Of the less studied drugs etoricoxib, 2.05 (1.45, 2.88), etodolac, 1.55 (1.28, 1.87), and indomethacin, 1.30 (1.19, 1.41), had the highest risks. In pair-wise comparisons, etoricoxib had a higher RR than ibuprofen, RRR = 1.68 (99% CI 1.14, 2.49), and naproxen, RRR = 1.75 (1.16, 2.64); etodolac was not significantly different from naproxen and ibuprofen. Naproxen had a significantly lower risk than ibuprofen, RRR = 0.92 (0.87, 0.99). RR estimates were constant with different background risks for cardiovascular disease and rose early in the course of treatment.
This review suggests that among widely used NSAIDs, naproxen and low-dose ibuprofen are least likely to increase cardiovascular risk. Diclofenac in doses available without prescription elevates risk. The data for etoricoxib were sparse, but in pair-wise comparisons this drug had a significantly higher RR than naproxen or ibuprofen. Indomethacin is an older, rather toxic drug, and the evidence on cardiovascular risk casts doubt on its continued clinical use. Please see later in the article for the Editors' Summary.
随机试验已经强调了大剂量和某些非典型情况下非甾体抗炎药(NSAIDs)的心血管风险。在这里,我们提供了在社区环境中使用典型剂量的个别 NSAIDs 的相对风险的估计值。
我们进行了一项基于社区的对照观察性研究的系统评价。我们进行了全面的文献搜索,提取了与使用个别 NSAIDs 相关的主要心血管事件的调整相对风险(RR)估计值,并对不同剂量和心血管事件低背景风险和高背景风险人群中的估计值进行了汇总。我们还在配对(within study)分析中比较了个别药物,生成了 RR 比(RRRs)。三十项病例对照研究包括 184946 例心血管事件,21 项队列研究描述了超过 270 万暴露人群的结局。在广泛研究的药物(十种或更多研究)中,罗非昔布的总体风险最高,为 1.45(95%CI 1.33,1.59),双氯芬酸为 1.40(1.27,1.55),而布洛芬最低,为 1.18(1.11,1.25),萘普生为 1.09(1.02,1.16)。在一组研究中,低剂量的罗非昔布、塞来昔布和双氯芬酸的风险升高,分别为 1.37(1.20,1.57)、1.26(1.09,1.47)和 1.22(1.12,1.33),并且每种药物的剂量越高,风险越高。布洛芬的风险仅在较高剂量时出现。萘普生在所有剂量下均无风险。较少研究的药物包括依托考昔、依托度酸和吲哚美辛,其风险最高,RR 分别为 2.05(1.45,2.88)、1.55(1.28,1.87)和 1.30(1.19,1.41)。在配对比较中,依托考昔的 RR 高于布洛芬,RRR=1.68(99%CI 1.14,2.49),萘普生,RRR=1.75(1.16,2.64);依托度酸与萘普生和布洛芬无显著差异。萘普生的风险明显低于布洛芬,RRR=0.92(0.87,0.99)。RR 估计值在不同的心血管疾病背景风险下保持不变,并在治疗早期上升。
本综述表明,在广泛使用的 NSAIDs 中,萘普生和低剂量布洛芬最不可能增加心血管风险。处方剂量的双氯芬酸会增加风险。依托考昔的数据较少,但在配对比较中,该药的 RR 明显高于萘普生或布洛芬。吲哚美辛是一种较老的、毒性较大的药物,其心血管风险的证据使其临床应用受到质疑。请稍后在文章中查看编辑摘要。