Department of Psychiatry, University of Zimbabwe, Harare, Zimbabwe.
BMC Public Health. 2011 Oct 26;11:828. doi: 10.1186/1471-2458-11-828.
There is limited evidence that interventions for depression and other common mental disorders (CMD) can be integrated sustainably into primary health care in Africa. We aimed to pilot a low-cost multi-component 'Friendship Bench Intervention' for CMD, locally adapted from problem-solving therapy and delivered by trained and supervised female lay workers to learn if was feasible and possibly effective as well as how best to implement it on a larger scale.
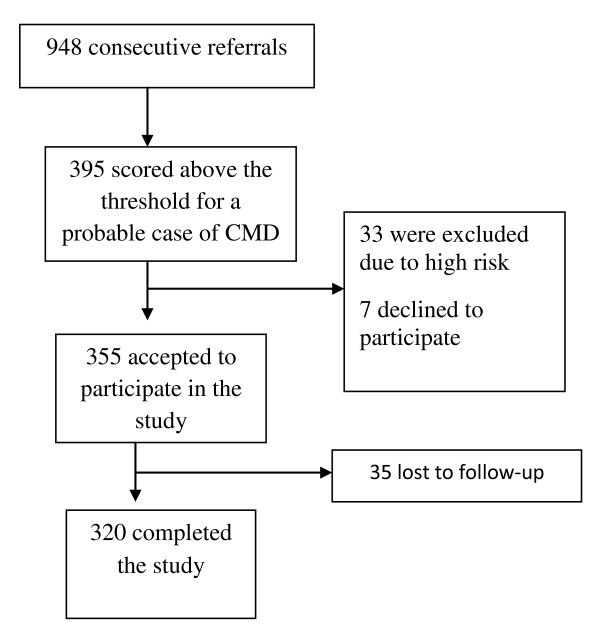
We trained lay workers for 8 days in screening and monitoring CMD and in delivering the intervention. Ten lay workers screened consecutive adult attenders who either were referred or self-referred to the Friendship Bench between July and December 2007. Those scoring above the validated cut-point of the Shona Symptom Questionnaire (SSQ) for CMD were potentially eligible. Exclusions were suicide risk or very severe depression. All others were offered 6 sessions of problem-solving therapy (PST) enhanced with a component of activity scheduling. Weekly nurse-led group supervision and monthly supervision from a mental health specialist were provided. Data on SSQ scores at 6 weeks after entering the study were collected by an independent research nurse. Lay workers completed a brief evaluation on their experiences of delivering the intervention.
Of 395 potentially eligible, 33 (8%) were excluded due to high risk. Of the 362 left, 2% (7) declined and 10% (35) were lost to follow-up leaving an 88% response rate (n = 320). Over half (n = 166, 52%) had presented with an HIV-related problem. Mean SSQ score fell from 11.3 (sd 1.4) before treatment to 6.5 (sd 2.4) after 3-6 sessions. The drop in SSQ scores was proportional to the number of sessions attended. Nine of the ten lay workers rated themselves as very able to deliver the PST intervention.
We have found preliminary evidence of a clinically meaningful improvement in CMD associated with locally adapted problem-solving therapy delivered by lay health workers through routine primary health care in an African setting. There is a need to test the effectiveness of this task-shifting mental health intervention in an appropriately powered randomised controlled trial.
ISRCTN: ISRCTN25476759.
有有限的证据表明,在非洲,将抑郁症和其他常见精神障碍(CMD)的干预措施可持续地纳入初级卫生保健中是可行的。我们旨在试点一种低成本的多成分“友谊长凳干预”(Friendship Bench Intervention),用于 CMD,该干预方案是在解决问题治疗的基础上进行了本地化调整,并由经过培训和监督的女性基层工作人员提供,以确定其在可行性和有效性方面是否可行,以及如何在更大规模上实施。
我们对基层工作人员进行了为期 8 天的培训,培训内容包括对 CMD 进行筛查和监测,以及提供干预措施。2017 年 7 月至 12 月,10 名基层工作人员对连续就诊的成年患者进行筛查,这些患者是由友谊长凳转介而来或自行前来就诊的。那些在经验证的绍纳症状问卷(Shona Symptom Questionnaire,SSQ)CMD 得分超过临界值的人有资格参与研究。排除标准为自杀风险或严重抑郁症。所有其他患者都被提供了 6 次解决问题治疗(Problem-solving therapy,PST),并辅以活动安排部分。每周由护士提供小组监督,每月由心理健康专家提供监督。由独立研究护士在进入研究后 6 周收集 SSQ 评分数据。基层工作人员对他们提供干预措施的经验进行了简短的评估。
在 395 名潜在合格的患者中,有 33 名(8%)因高风险而被排除。在剩下的 362 名患者中,有 2%(7 名)拒绝,10%(35 名)失访,因此回应率为 88%(n=320)。超过一半的患者(n=166,52%)因与艾滋病毒相关的问题就诊。SSQ 评分从治疗前的 11.3(标准差 1.4)降至治疗后 3-6 次后的 6.5(标准差 2.4)。SSQ 评分的下降与就诊次数成正比。10 名基层工作人员中有 9 名自我评估为能够非常有效地提供 PST 干预措施。
我们初步发现,在非洲常规初级卫生保健环境中,通过基层卫生工作者提供的本地化调整后的解决问题治疗,可以显著改善与 CMD 相关的临床症状。需要在适当的随机对照试验中检验这种转移精神卫生干预措施的有效性。
ISRCTN:ISRCTN53032137。