Special Programme for Research and Training in Tropical Diseases (TDR_WHO), Geneva, Switzerland.
Pathog Glob Health. 2012 May;106(2):94-101. doi: 10.1179/2047773212Y.0000000017.
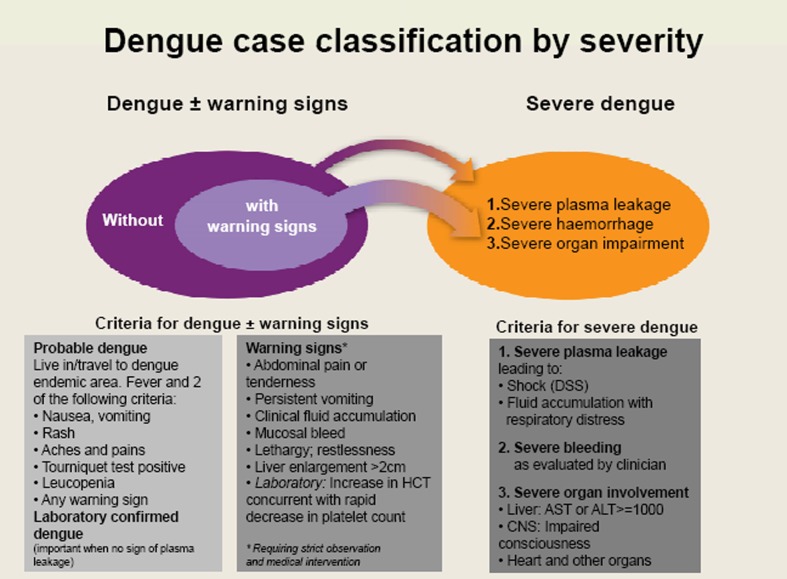
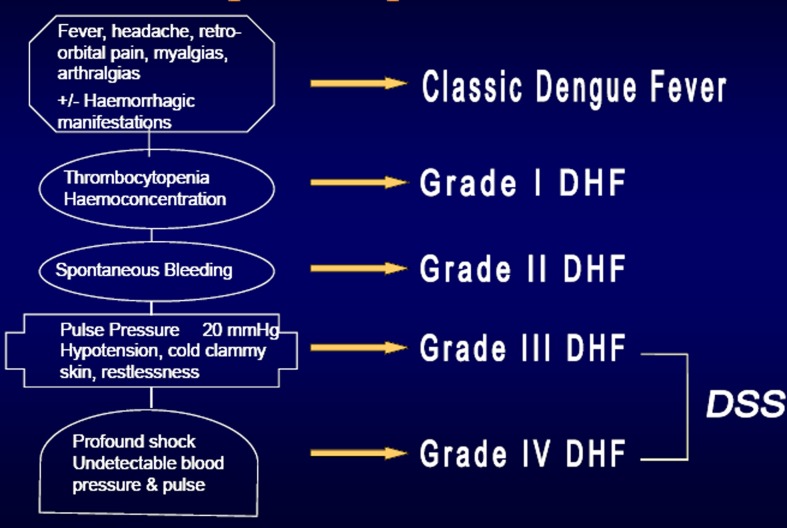
With the example of dengue, an evidence-based approach to prospectively develop a case classification is described, gathering evidence for identifying strength and weaknesses of the existing model, collecting new data describing the disease as it occurs globally, further developing a new model that can be applied in practice and field testing the newly developed model in comparison to the previous model. For each step in this process, the highest available level of evidence has been applied. This process has been initiated by the World Health Organization's (WHO) Special Programme for Research and Training in Tropical Diseases (TDR) and WHO's Department for Control of Neglected Tropical Diseases (NTD), developing the following for dengue. Since the early 1970s, dengue has been classified into dengue fever, dengue haemorrhagic fever grades I and II and dengue shock syndrome grades III and IV (DF/DHF/DSS). However, in recent years, a growing number of dengue clinicians have questioned the shortcomings of this scheme. The issues have revolved around the complexity of confirming DHF in clinical practice, misclassifying severe cases as DF, and the emphasis on haemorrhage rather than plasma leakage as the underlying problem in most severe dengue cases. Step 1: A systematic literature review highlighted the shortcomings of the DF/DHF/DSS scheme: (1) difficulties in applying the criteria for DHF/DSS; (2) the tourniquet test has a low sensitivity for distinguishing between DHF and DF; and (3) most DHF criteria had a large variability in frequency of occurrence. Step 2: An analysis of regional and national dengue guidelines and their application in the clinical practice showed a need to re-evaluate and standardize guidelines as the actual ones showed a large variation of definitions, an inconsistent application by medical staff, and a lack of diagnostic facilities necessary for the DHF diagnosis in frontline services. Step 3: A prospective cohort study in seven countries, confirmed the difficulties in applying the DF/DHF/DSS criteria even in tertiary care hospitals, that DF/DHF/DSS do not represent levels of disease severity and that a clear distinction between severe dengue (defined by plasma leakage and/or severe haemorrhage, and/or organ failure) and (non-severe) dengue can be made using highly sensitive and specific criteria. In contrast, the sub-grouping of (non-severe) dengue into two further severity levels was only possible with criteria that gave approximately 70% sensitivity and specificity. Step 4: Three regional expert consensus groups in the Americas and Asia concluded that 'dengue is one disease entity with different clinical presentations and often with unpredictable clinical evolution and outcome' and that, revising the results of Step 3, DF/DHF/DSS is not related to disease severity. Step 5: In a global expert consensus meeting at WHO in Geneva/Switzerland the evidence collected in Steps 1-4 was reviewed and a revised scheme was developed and accepted, distinguishing: dengue with or without warning signs and severe dengue; the further field testing and acquisition of further prospective evidence of the revised scheme was recommended. Step 6: In 18 countries, the usefulness and applicability of the revised classification compared to the DF/DHF/DSS scheme were tested showing clear results in favour of the revised classification. Step 7: Studies are under way on the predictive value of warning signs for severe dengue and on criteria for the clinical diagnosis of dengue which will complete the evidence foundation of the revised classification. The analysis has shown that the revised dengue case classification is better able to standardize clinical management, raise awareness about unnecessary interventions, match patient categories with specific treatment instructions, and make the key messages of patient management understandable for all health care staff dealing with dengue patients. Furthermore, the evidence-based approach to develop prospectively the dengue case classification could be a model approach for other disease classifications.
以登革热为例,描述了一种基于证据的前瞻性病例分类方法,该方法旨在收集证据,以确定现有模型的优势和劣势,收集描述全球疾病发生情况的新数据,进一步开发可在实践中应用的新模型,并将新开发的模型与之前的模型进行现场测试。在这个过程的每一步中,都应用了最高级别的现有证据。这一过程是由世界卫生组织(WHO)热带病研究与培训特别规划署(TDR)和 WHO 控制被忽视热带病司(NTD)发起的,为登革热制定了以下方案。自 20 世纪 70 年代初以来,登革热一直分为登革热、登革出血热 I 级和 II 级以及登革休克综合征 III 级和 IV 级(DF/DHF/DSS)。然而,近年来,越来越多的登革热临床医生对该方案的缺点提出了质疑。这些问题主要集中在确认 DHF 临床实践的复杂性、将严重病例误诊为 DF、以及强调出血而不是血浆渗漏是大多数严重登革热病例的根本问题上。步骤 1:系统文献回顾突出了 DF/DHF/DSS 方案的缺点:(1)应用 DHF/DSS 标准的困难;(2)止血带试验对区分 DHF 和 DF 的敏感性较低;(3)大多数 DHF 标准的发生频率差异较大。步骤 2:对区域和国家登革热指南及其在临床实践中的应用进行分析表明,需要重新评估和标准化指南,因为实际指南在定义、医务人员的不一致应用以及前线服务中进行 DHF 诊断所需的诊断设施方面存在较大差异。步骤 3:在七个国家进行的前瞻性队列研究证实,即使在三级保健医院,应用 DF/DHF/DSS 标准也存在困难,DF/DHF/DSS 并不代表疾病严重程度,并且可以使用高度敏感和特异的标准来区分严重登革热(定义为血浆渗漏和/或严重出血,和/或器官衰竭)和(非严重)登革热。相比之下,使用大约 70%的灵敏度和特异性的标准,只能将(非严重)登革热分为两个进一步的严重程度级别。步骤 4:美洲和亚洲的三个区域专家共识小组得出结论,“登革热是一种具有不同临床表现的疾病实体,常常具有不可预测的临床演变和结果”,并修订了第 3 步的结果,DF/DHF/DSS 与疾病严重程度无关。步骤 5:在瑞士日内瓦世卫组织举行的一次全球专家共识会议上,审查了在步骤 1-4 中收集的证据,并制定并接受了一个修订方案,区分:有或没有预警信号的登革热和严重登革热;建议进一步现场测试和获取修订方案的前瞻性证据。步骤 6:在 18 个国家,对修订后的分类与 DF/DHF/DSS 方案的有用性和适用性进行了测试,结果明显有利于修订后的分类。步骤 7:正在对预警信号对严重登革热的预测价值以及登革热的临床诊断标准进行研究,这将完善修订后的分类的证据基础。分析表明,修订后的登革热病例分类能够更好地规范临床管理,提高对不必要干预的认识,将患者类别与特定治疗说明相匹配,并使所有处理登革热患者的医护人员都能理解患者管理的关键信息。此外,前瞻性开发登革热病例分类的循证方法可以成为其他疾病分类的一种模式方法。