Department of Health Systems Financing, World Health Organization, avenue appia 20, Geneva, Switzerland.
BMJ. 2012 Mar 2;344:e612. doi: 10.1136/bmj.e612.
To identify and estimate the population costs and effects of a selected set of enforcement strategies for reducing the burden of road traffic injuries in developing countries.
Cost effectiveness analysis based on an epidemiological model.
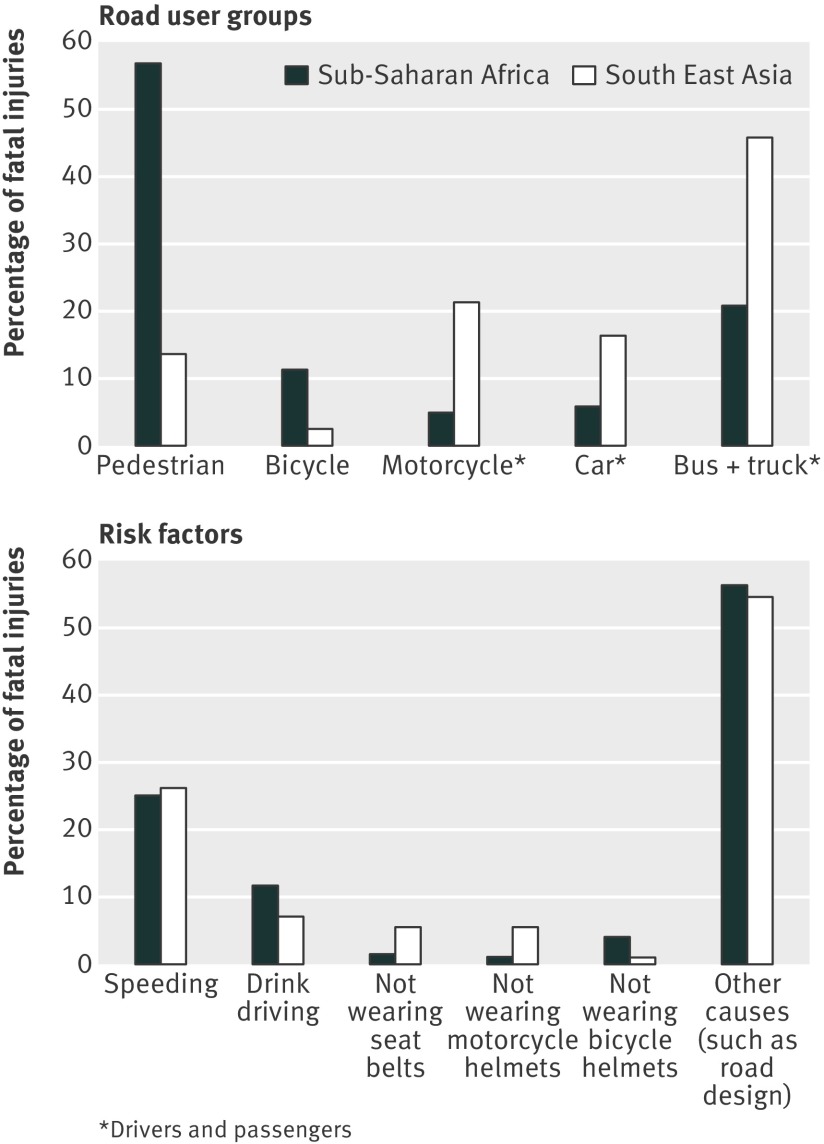
Two epidemiologically defined World Health Organization sub-regions of the world: countries in sub-Saharan Africa with very high adult and high child mortality (AfrE); and countries in South East Asia with high adult and high child mortality (SearD).
Enforcement of speed limits via mobile speed cameras; drink-drive legislation and enforcement via breath testing campaigns; legislation and primary enforcement of seatbelt use in cars; legislation and enforcement of helmet use by motorcyclists; legislation and enforcement of helmet use by bicyclists.
Patterns of injury were fitted to a state transition model to determine the expected population level effects of intervention over a 10 year period, which were expressed in disability adjusted life years (DALYs) averted. Costs were expressed in international dollars ($Int) for the year 2005.
The single most cost effective strategy varies by sub-region, but a combined intervention strategy that simultaneously enforces multiple road safety laws produces the most health gain for a given amount of investment. For example, the combined enforcement of speed limits, drink-driving laws, and motorcycle helmet use saves one DALY for a cost of $Int1000-3000 in the two sub-regions considered.
The potential impact of available road safety measures is inextricably bound by the underlying distribution of road traffic injuries across different road user groups and risk factors. Combined enforcement strategies are expected to represent the most efficient way to reduce the burden of road traffic injuries, because they benefit from considerable synergies on the cost side while generating greater overall health gains.
确定并评估一系列有选择的执法策略的人群成本和效果,以减轻发展中国家道路交通伤害的负担。
基于流行病学模型的成本效益分析。
世界卫生组织两个流行病学定义的亚区域:撒哈拉以南非洲国家,成人和儿童死亡率非常高(AfrE);东南亚国家,成人和儿童死亡率高(SearD)。
通过移动速度相机执行限速;通过呼气测试运动执行酒后驾车立法和执法;立法并主要执行汽车安全带使用;立法并执行摩托车手头盔使用;立法并执行自行车手头盔使用。
损伤模式拟合到状态转移模型,以确定干预在 10 年内对人群水平的预期效果,以避免的残疾调整生命年(DALY)表示。成本以 2005 年的国际美元($Int)表示。
最具成本效益的策略因亚区而异,但同时执行多项道路安全法的综合干预策略可在给定投资额度内获得最大的健康收益。例如,在考虑的两个亚区中,同时执行限速、酒后驾车法和摩托车头盔使用的综合执法可节省 1 个 DALY,成本为$Int1000-3000。
可用道路安全措施的潜在影响与不同道路使用者群体和危险因素之间道路交通伤害的基本分布密不可分。综合执法策略有望成为减轻道路交通伤害负担的最有效方式,因为它们在成本方面具有相当大的协同作用,同时产生更大的整体健康收益。