School of Medicine and Health Sciences, Universidad del Rosario, Bogotá, Colombia.
BMJ. 2012 Mar 2;344:e607. doi: 10.1136/bmj.e607.
To determine the relative costs and health effects of interventions to combat cardiovascular disease, diabetes, and tobacco related disease in order to guide the allocation of resources in developing countries.
Cost effectiveness analysis of 123 single or combined prevention and treatment strategies for cardiovascular disease, diabetes, and smoking by means of a lifetime population model.
Two World Health Organization sub-regions of the world: countries in sub-Saharan Africa with very high adult and high child mortality (AfrE) and countries in South East Asia with high adult and high child mortality (SearD).
Demographic and epidemiological data were taken from the WHO databases of mortality and global burden of disease. Estimates of intervention coverage, effectiveness, and resource needs were drawn from clinical trials, observational studies, and treatment guidelines. Unit costs were taken from the WHO-CHOICE (Choosing Interventions that are Cost-Effective) price database.
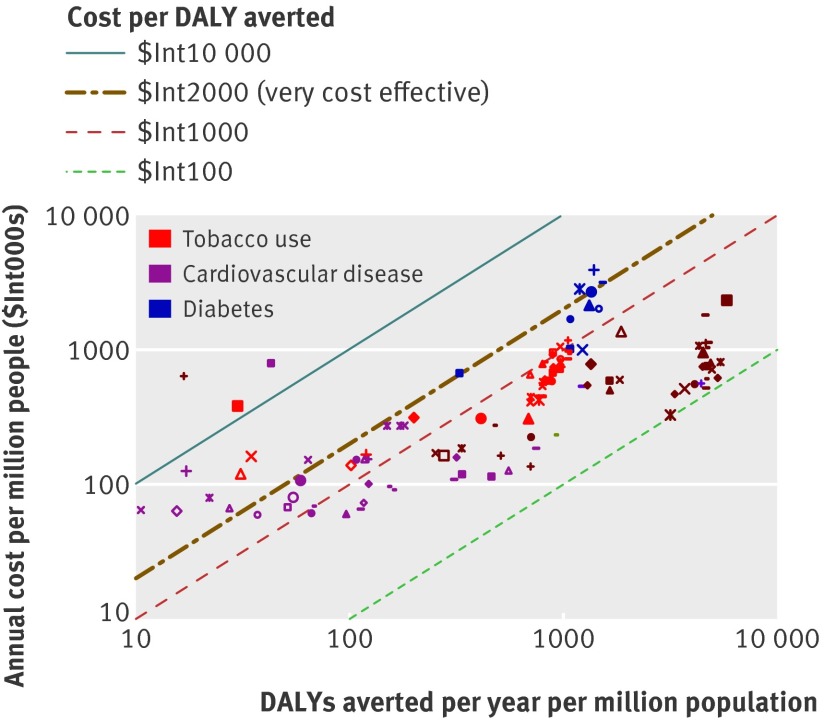
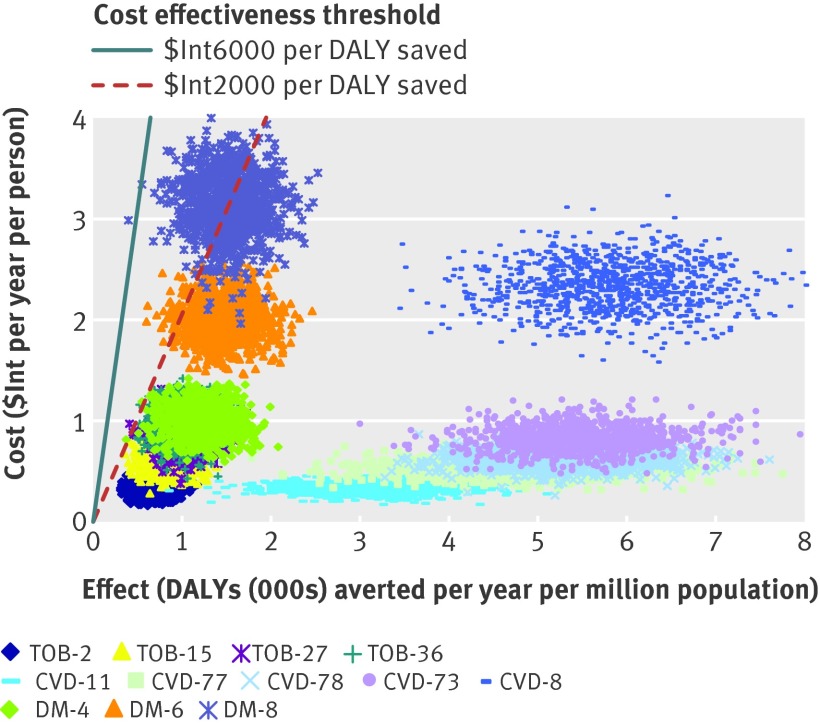
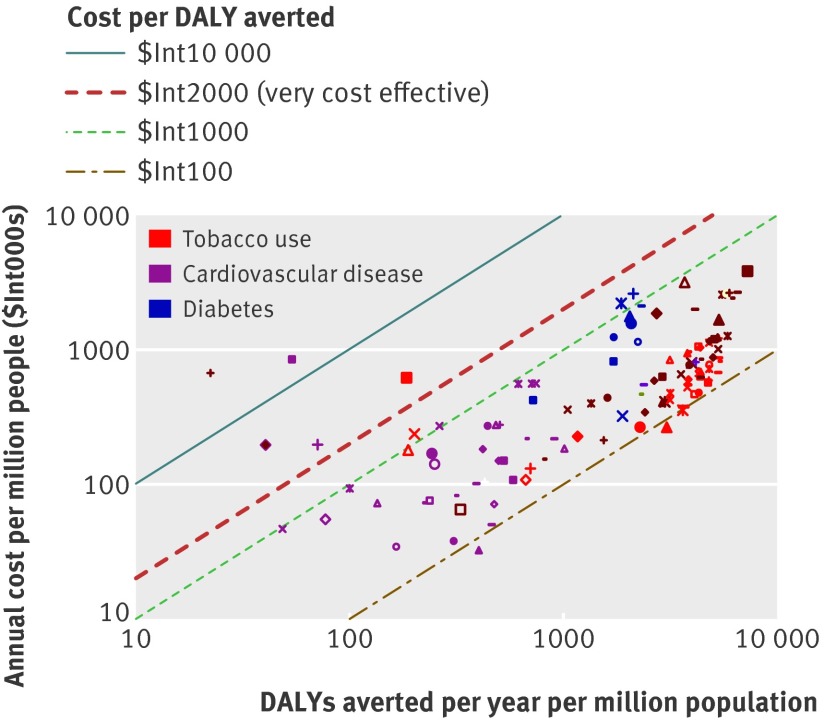
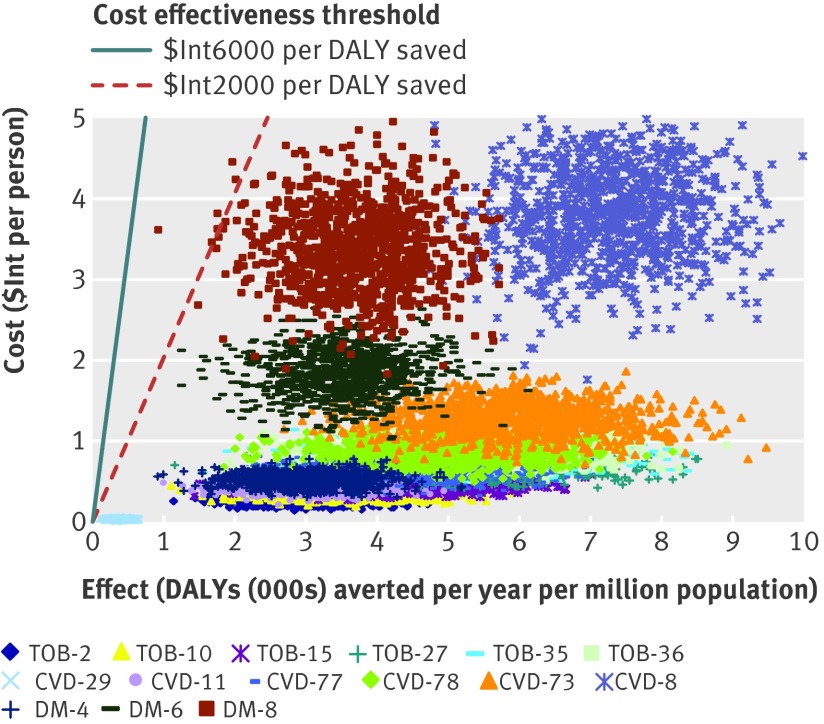
Cost per disability adjusted life year (DALY) averted, expressed in international dollars ($Int) for the year 2005.
Most of the interventions studied were considered highly cost effective, meaning they generate one healthy year of life at a cost of <$Int2000 (which is the gross domestic product per capita of the two regions considered here). Interventions that offer particularly good monetary value, and which could be considered for prioritised implementation or scale up, include demand reduction strategies of the Framework Convention for Tobacco Control (<$Int950 and <$Int200 per DALY averted in AfrE and SearD respectively); combination drug therapy for people with a >25% chance of experiencing a cardiovascular event over the next decade, either alone or together with specific multidrug regimens for the secondary prevention of post-acute ischaemic heart disease and stroke (<$Int150 and <$Int230 per DALY averted in AfrE and SearD respectively); and retinopathy screening and glycaemic control for patients with diabetes (<$Int2100 and <$Int950 per DALY averted in AfrE and SearD respectively).
This comparative economic assessment has identified a set of population-wide and individual strategies for prevention and control of cardiovascular disease that are inexpensive and cost effective in low resource settings.
确定对抗心血管疾病、糖尿病和烟草相关疾病的干预措施的相对成本和健康效果,以指导发展中国家资源的分配。
通过终生人群模型对心血管疾病、糖尿病和吸烟的 123 种单一或联合预防和治疗策略进行成本效益分析。
世界卫生组织的两个次区域:撒哈拉以南非洲地区(成人和儿童死亡率极高的国家,简称 AfrE)和东南亚地区(成人和儿童死亡率高的国家,简称 SearD)。
人口统计和流行病学数据取自世卫组织死亡率数据库和全球疾病负担数据库。干预措施覆盖率、效果和资源需求的估计值来自临床试验、观察性研究和治疗指南。单位成本取自世卫组织 CHOICE(选择具有成本效益的干预措施)价格数据库。
每避免一个残疾调整生命年(DALY)的成本,以 2005 年的国际元($Int)表示。
研究中的大多数干预措施被认为具有很高的成本效益,这意味着它们以低于$Int2000(这是两个考虑区域的人均国内生产总值)的成本产生一年健康寿命。具有特别高货币价值且可优先实施或扩大规模的干预措施包括《烟草控制框架公约》的需求减少战略(AfrE 和 SearD 中分别为<$Int950 和<$Int200 每 DALY 避免);单独或与用于二级预防急性缺血性心脏病和中风后特定多药方案联合使用的治疗药物,对未来十年内有>25%机会经历心血管事件的患者进行联合药物治疗(AfrE 和 SearD 中分别为<$Int150 和<$Int230 每 DALY 避免);以及对糖尿病患者进行视网膜病变筛查和血糖控制(AfrE 和 SearD 中分别为<$Int2100 和<$Int950 每 DALY 避免)。
这项比较性经济评估确定了一系列用于心血管疾病预防和控制的人群和个体策略,在资源有限的环境中,这些策略既便宜又具有成本效益。