Clinical Nutrition and Risk Factor Modification Centre, St. Michael’s Hospital, Toronto, ON, Canada.
J Nutr. 2012 May;142(5):916-23. doi: 10.3945/jn.111.151951. Epub 2012 Mar 28.
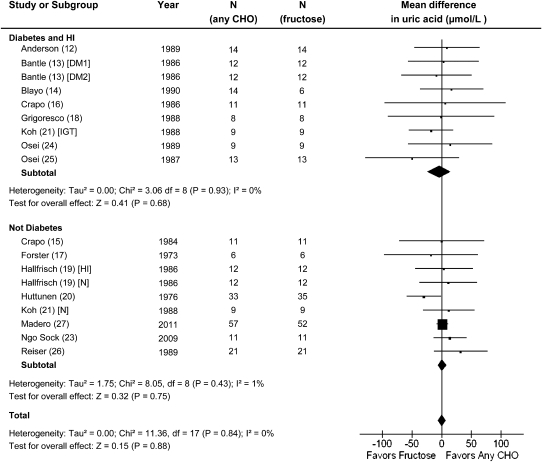
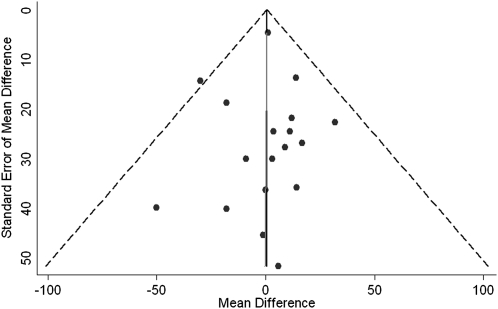
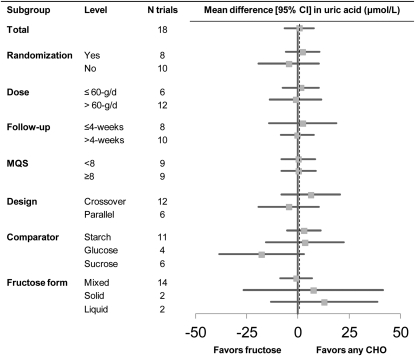
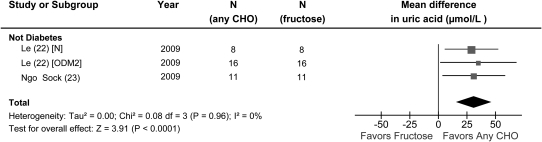
Hyperuricemia is linked to gout and features of metabolic syndrome. There is concern that dietary fructose may increase uric acid concentrations. To assess the effects of fructose on serum uric acid concentrations in people with and without diabetes, we conducted a systematic review and meta-analysis of controlled feeding trials. We searched MEDLINE, EMBASE, and the Cochrane Library for relevant trials (through August 19, 2011). Analyses included all controlled feeding trials ≥ 7 d investigating the effect of fructose feeding on uric acid under isocaloric conditions, where fructose was isocalorically exchanged with other carbohydrate, or hypercaloric conditions, and where a control diet was supplemented with excess energy from fructose. Data were aggregated by the generic inverse variance method using random effects models and expressed as mean difference (MD) with 95% CI. Heterogeneity was assessed by the Q statistic and quantified by I(2). A total of 21 trials in 425 participants met the eligibility criteria. Isocaloric exchange of fructose for other carbohydrate did not affect serum uric acid in diabetic and nondiabetic participants [MD = 0.56 μmol/L (95% CI: -6.62, 7.74)], with no evidence of inter-study heterogeneity. Hypercaloric supplementation of control diets with fructose (+35% excess energy) at extreme doses (213-219 g/d) significantly increased serum uric acid compared with the control diets alone in nondiabetic participants [MD = 31.0 mmol/L (95% CI: 15.4, 46.5)] with no evidence of heterogeneity. Confounding from excess energy cannot be ruled out in the hypercaloric trials. These analyses do not support a uric acid-increasing effect of isocaloric fructose intake in nondiabetic and diabetic participants. Hypercaloric fructose intake may, however, increase uric acid concentrations. The effect of the interaction of energy and fructose remains unclear. Larger, well-designed trials of fructose feeding at "real world" doses are needed.
高尿酸血症与痛风和代谢综合征的特征有关。人们担心饮食中的果糖可能会增加尿酸浓度。为了评估果糖对糖尿病患者和非糖尿病患者血清尿酸浓度的影响,我们对对照喂养试验进行了系统评价和荟萃分析。我们检索了 MEDLINE、EMBASE 和 Cochrane Library 中相关的试验(截至 2011 年 8 月 19 日)。分析包括所有对照喂养试验,这些试验研究了在等热量条件下果糖喂养对尿酸的影响,在等热量条件下,果糖与其他碳水化合物等热量交换,或在高热量条件下,对照饮食中添加了过量的果糖能量。数据通过随机效应模型的通用逆方差法进行汇总,并以均数差值(MD)和 95%置信区间(CI)表示。通过 Q 统计量评估异质性,并通过 I(2)进行量化。共有 21 项试验涉及 425 名参与者,符合入选标准。在糖尿病患者和非糖尿病患者中,果糖与其他碳水化合物等热量交换并不影响血清尿酸[MD = 0.56 μmol/L(95%CI:-6.62,7.74)],且无研究间异质性。在非糖尿病患者中,与单独对照饮食相比,极端剂量(213-219 g/d)的果糖对对照饮食的高能量补充(+35%的能量过剩)显著增加了血清尿酸[MD = 31.0 mmol/L(95%CI:15.4,46.5)],且无异质性。在高能量试验中,不能排除多余能量的混杂作用。这些分析结果不支持非糖尿病和糖尿病患者等热量果糖摄入会增加尿酸的假说。然而,高能量的果糖摄入可能会增加尿酸浓度。能量和果糖相互作用的影响仍不清楚。需要进行更大规模、设计良好的果糖喂养“真实世界”剂量试验。