Department of Rheumatology, VU University Medical Center, Amsterdam, The Netherlands.
Curr Rheumatol Rep. 2012 Jun;14(3):224-30. doi: 10.1007/s11926-012-0252-8.
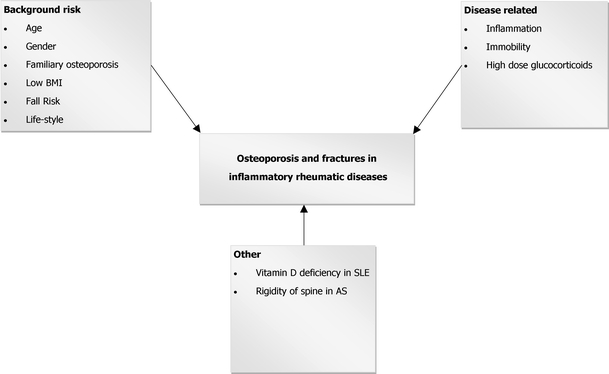
Inflammatory joint diseases such as rheumatoid arthritis, as well as other rheumatic conditions, such as systemic lupus erythematosus (SLE) and ankylosing spondylitis, comprise a heterogeneous group of joint disorders that are all associated with extra-articular side effects, including bone loss and fractures. The concept of osteoimmunology is based on growing insights into the links between the immune system and bone. The pathogenesis of osteoporosis in these patients is multifactorial. We have, more or less as an example, described this extensively for patients with SLE. High disease activity (inflammation) and immobility are common factors that substantially increase fracture risk in these patients, on top of the background fracture risk based on, among other factors, age, body mass index, and gender. Although no fracture reduction has been shown in intervention studies in patients with inflammatory rheumatic diseases, we present treatment options that might be useful for clinicians who are treating these patients.
炎性关节疾病,如类风湿关节炎,以及其他风湿性疾病,如系统性红斑狼疮(SLE)和强直性脊柱炎,构成了一组异质性的关节疾病,它们都与关节外的副作用有关,包括骨质流失和骨折。骨免疫学的概念是基于对免疫系统和骨骼之间联系的深入了解。这些患者骨质疏松症的发病机制是多因素的。我们已经或多或少地详细描述了 SLE 患者的情况。高疾病活动度(炎症)和活动受限是这些患者骨折风险显著增加的常见因素,除此之外,还有其他因素,如年龄、体重指数和性别等,也会增加骨折风险。虽然在炎性风湿性疾病患者的干预研究中没有显示出骨折减少,但我们提出了一些治疗选择,这些选择可能对治疗这些患者的临床医生有用。