Clark Brian T, Garcia-Tsao Guadalupe, Fraenkel Liana
Veterans Administration, Connecticut Healthcare System, West Haven.
Patient Prefer Adherence. 2012;6:285-95. doi: 10.2147/PPA.S30111. Epub 2012 Apr 4.
Guidelines for hepatitis C (HCV) strongly recommend antiviral treatment for patients with more severe liver disease given their increased risk of developing cirrhosis and other liver-related complications. Despite the proven benefits of therapy, 70%-88% of patients chronically infected with HCV do not undergo treatment. The goal of this paper is to describe patterns of treatment initiation among patients with both mild and severe disease and to assess the factors that are associated with treatment initiation and completion.
Subjects completed previously validated questionnaires to ascertain sociodemographic characteristics, choice predisposition, and clinical characteristics prior to meeting with the hepatologist to discuss treatment initiation and were followed for 12 months. We examined the association between patient characteristics and treatment patterns controlling for liver disease severity.
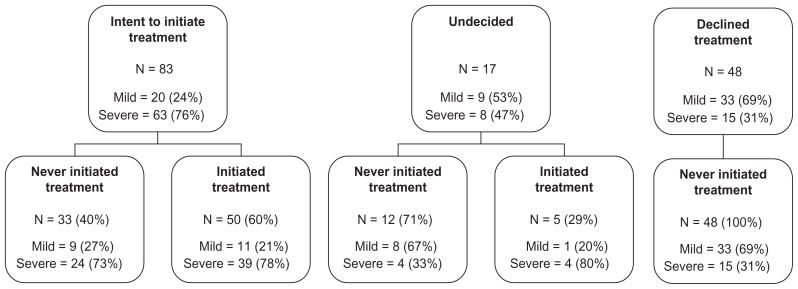
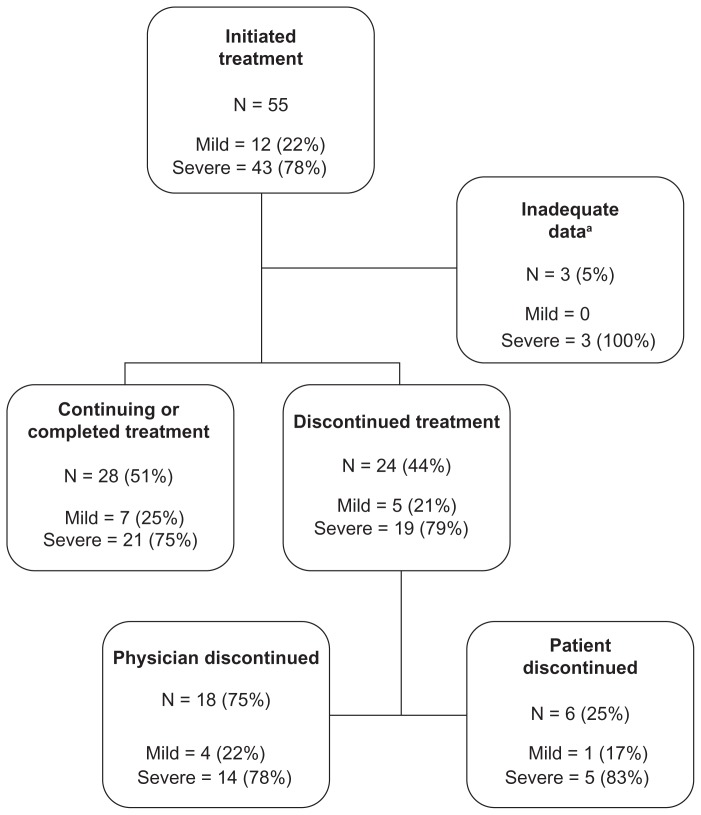
Of the 148 eligible subjects entered into our study, 55 (37%) initiated treatment during the 12-month follow-up period. Of the 86 subjects with severe liver disease, 43 (50%) initiated treatment. Financial barriers and geographic access to care were the most common reasons for treatment deferral. Of the 55 patients initiating treatment, 24 (44%) discontinued treatment, with intolerance of side effects being the most common reason for discontinuation. After adjusting for liver disease severity, patient choice predisposition (prior to discussion with their provider) was strongly associated with initiation of treatment, while sociodemographic characteristics were not.
Treatment initiation did align with current recommendations (patients with severe disease were more likely to initiate treatment), however, rates of treatment initiation and completion were low. Patient choice predisposition is the strongest predictor of treatment initiation, independent of disease severity. Improving individualized treatment outcomes for patients with chronic HCV requires efforts at identifying patients' choice predisposition, and improving access for those wishing to initiate therapy.
丙型肝炎(HCV)指南强烈建议,患有更严重肝病的患者接受抗病毒治疗,因为他们发展为肝硬化和其他肝脏相关并发症的风险增加。尽管治疗已被证明有益,但70%-88%的慢性丙型肝炎病毒感染者未接受治疗。本文的目的是描述轻度和重度疾病患者的治疗起始模式,并评估与治疗起始和完成相关的因素。
受试者在与肝病专家会面讨论治疗起始之前,完成了先前经过验证的问卷,以确定社会人口学特征、选择倾向和临床特征,并随访12个月。我们研究了患者特征与控制肝病严重程度的治疗模式之间的关联。
在纳入我们研究的148名符合条件的受试者中,55名(37%)在12个月的随访期内开始治疗。在86名患有严重肝病的受试者中,43名(50%)开始治疗。经济障碍和获得医疗服务的地理便利性是推迟治疗的最常见原因。在开始治疗的55名患者中,24名(44%)停止治疗,副作用不耐受是停止治疗的最常见原因。在调整肝病严重程度后,患者的选择倾向(在与医疗服务提供者讨论之前)与治疗起始密切相关,而社会人口学特征则不然。
治疗起始确实与当前建议一致(重症患者更有可能开始治疗),然而,治疗起始率和完成率较低。患者的选择倾向是治疗起始的最强预测因素,与疾病严重程度无关。改善慢性丙型肝炎患者的个体化治疗结果需要努力识别患者的选择倾向,并改善那些希望开始治疗的患者的就医机会。