Perinatal and Reproductive Epidemiology Research Unit, The University of New South Wales, Level 2, McNevin Dickson Building, Randwick Hospitals Campus, Sydney 2031, Australia.
BMC Health Serv Res. 2012 Jun 8;12:142. doi: 10.1186/1472-6963-12-142.
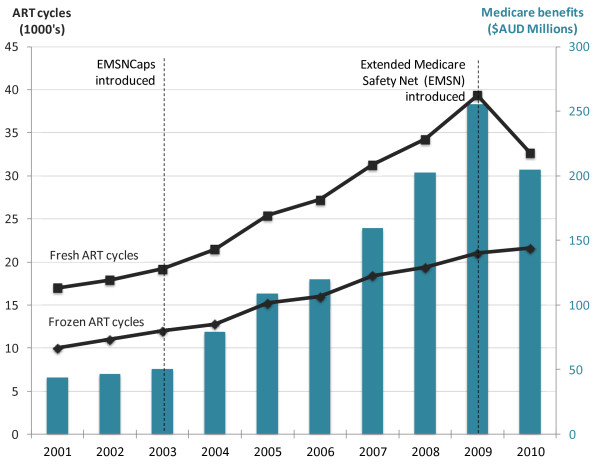
Almost all assisted reproductive technology (ART) and intrauterine insemination (IUI) treatments performed in Australia are subsidized through the Australian Government's universal insurance scheme, Medicare. In 2010 restrictions on the amount Medicare paid in benefits for these treatments were introduced, increasing patient out-of-pocket payments for fresh and frozen embryo ART cycles and IUI. The aim of this study was to evaluate the impact of the policy on access to treatment, savings in Medicare benefits and the number of ART conceived children not born.
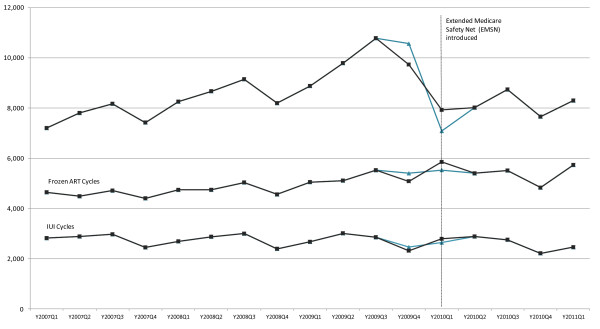
Pooled quarterly cross-sectional Medicare data from 2007 and 2011 where used to construct a series of Ordinary Least Squares (OLS) regression models to evaluate the impact of the policy on access to treatment by women of different ages. Government savings in the 12 months after the policy was calculated as the difference between the predicted and observed Medicare benefits paid.
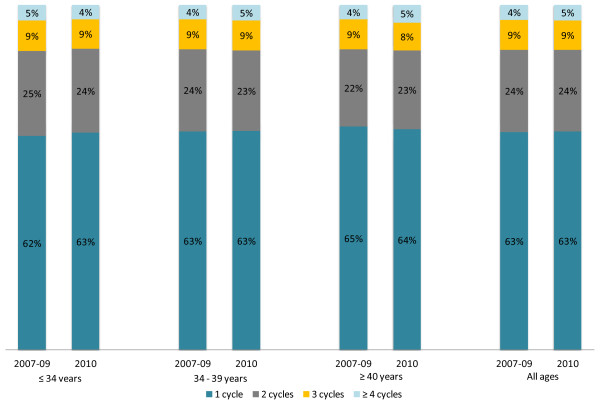
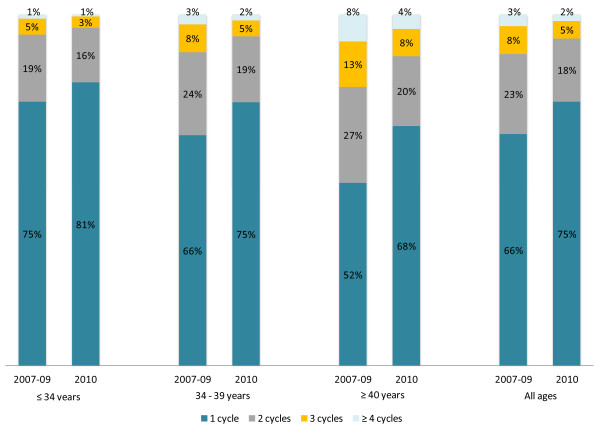
After controlling for underlying time trends and unobserved factors the policy change reduced the number of fresh embryo cycles by almost 8600 cycles over 12 months (a 16% reduction in cycles, p < 0.001). The policy effect was greatest on women aged 40 years and older (38% reduction in cycles, p < 0.001). Younger women engaged in relatively more anticipatory behaviour by bringing forward their fresh cycles to 2009. Frozen embryo cycles, which are approximately one quarter of the cost of a fresh cycle, were only marginally impacted by the policy. Utilisation of IUI cycles were not impacted by the policy. After adjusting for anticipatory behaviour, $76 million in Medicare benefits was saved in the 12 months after the policy change (0.47% of annual Medicare benefits). Between 1200 and 1500 ART conceived children were not born in 2010 as a consequence of the policy.
The introduction of the policy resulted in a significant reduction in fresh ART cycles in the first 15 months after its introduction. Further evaluation on the long-term impact of the policy with regard access to treatment and on clinical practice, particularly the number of embryos transferred, is crucial to ensuring equitable access to fertility treatment and the health and welfare of ART children.
在澳大利亚,几乎所有的辅助生殖技术(ART)和宫腔内人工授精(IUI)治疗都通过澳大利亚政府的全民医疗保险计划 Medicare 来补贴。2010 年,对这些治疗的 Medicare 报销金额进行了限制,增加了新鲜和冷冻胚胎 ART 周期以及 IUI 的患者自费支付额。本研究旨在评估该政策对治疗机会、医疗保险节省和未出生的 ART 受孕儿童数量的影响。
使用 2007 年和 2011 年的 Medicare 季度汇总横断面数据构建一系列普通最小二乘(OLS)回归模型,以评估该政策对不同年龄段女性获得治疗的影响。政策实施后 12 个月内的政府节省额计算为预测和实际 Medicare 报销金额之间的差值。
在控制潜在的时间趋势和未观察到的因素后,该政策变化导致 12 个月内新鲜胚胎周期减少了近 8600 个周期(周期减少 16%,p<0.001)。该政策对 40 岁及以上的女性影响最大(周期减少 38%,p<0.001)。年轻女性通过提前到 2009 年进行新鲜周期来进行更多的预期行为。冷冻胚胎周期,其成本约为新鲜周期的四分之一,仅受到政策的轻微影响。IUI 周期的使用不受政策影响。调整预期行为后,政策变化后 12 个月内 Medicare 节省了 7600 万美元(占 Medicare 年度支出的 0.47%)。由于该政策,2010 年有 1200 至 1500 名 ART 受孕儿童未出生。
该政策的实施导致其实施后的头 15 个月内新鲜 ART 周期显著减少。进一步评估该政策对治疗机会和临床实践的长期影响,特别是胚胎移植数量,对于确保公平获得生育治疗以及 ART 儿童的健康和福利至关重要。