Department of Gastroenterology, Pulido Valente Hospital, Lisbon, Portugal.
BMC Gastroenterol. 2012 Jun 12;12:70. doi: 10.1186/1471-230X-12-70.
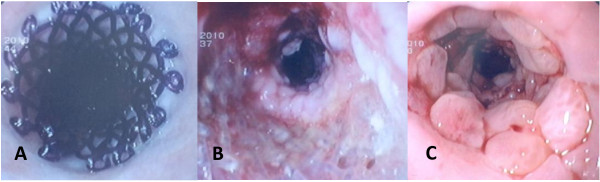
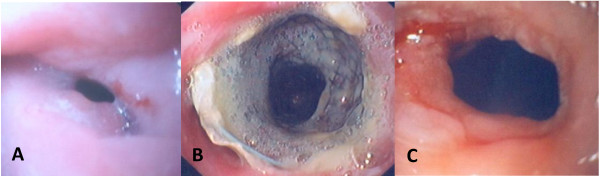
Refractory benign esophageal strictures (RBESs) have been treated with the temporary placement of different self-expanding stents with conflicting results. We compared the clinical effectiveness of 3 types of stents: self-expanding plastic stents (SEPSs), biodegradable stents, and fully covered self-expanding metal stents (FCSEMSs), for the treatment of RBES.
This study prospectively evaluated 3 groups of 30 consecutive patients with RBESs who underwent temporary placement of either SEPSs (12 weeks, n = 10), biodegradable stents (n = 10) or FCSEMSs (12 weeks, n = 10). Data were collected to analyze the technical success and clinical outcome of the stents as evaluated by recurrent dysphagia, complications and reinterventions.
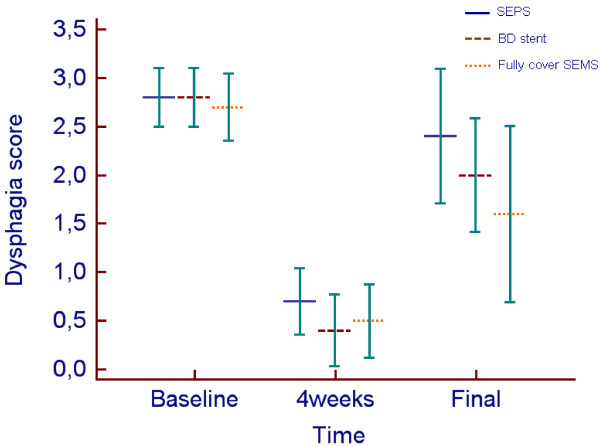
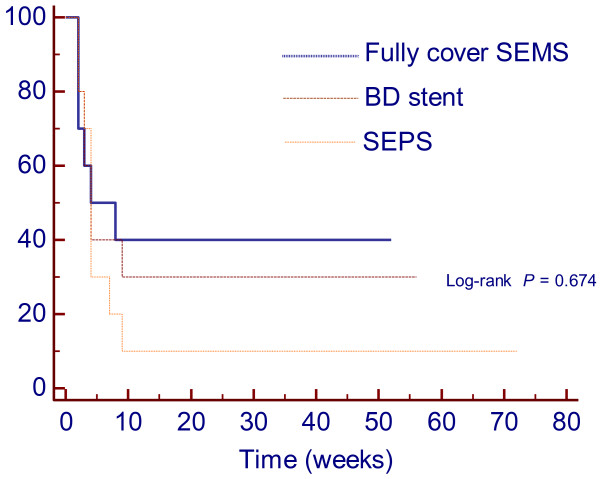
Stent implantation was technically successful in all patients. Migration occurred in 11 patients: 6 (60%) in the SEPS group, 2 (20%) in the biodegradable group and 3 (30%) in the FCSEMS group (P = 0.16). A total of 8/30 patients (26.6%) were dysphagia-free after the end of follow-up: 1 (10%) in the SEPS group, 3 (30%) in the biodegradable group and 4 (40%) in the FCSEMS group (P = 0.27). More reinterventions were required in the SEPS group (n = 24) than in the biodegradable group (n = 13) or the FCSEMS group (n = 13) (P = 0.24). Multivariate analysis showed that stricture length was significantly associated with higher recurrence rates after temporary stent placement (HR = 1.37; 95% CI = 1.08-1.75; P = 0.011).
Temporary placement of a biodegradable stent or of a FCSEMS in patients with RBES may lead to long-term relief of dysphagia in 30 and 40% of patients, respectively. The use of SEPSs seems least preferable, as they are associated with frequent stent migration, more reinterventions and few cases of long-term improvement. Additionally, longer strictures were associated with a higher risk of recurrence.
难治性良性食管狭窄(RBES)曾采用不同的自膨式支架进行临时放置治疗,但结果不一。我们比较了 3 种支架(自膨式塑料支架、生物可降解支架和全覆膜自膨式金属支架)治疗 RBES 的临床疗效。
本研究前瞻性纳入 3 组连续 30 例 RBES 患者,分别行自膨式塑料支架(12 周,n=10)、生物可降解支架(n=10)或全覆膜自膨式金属支架(12 周,n=10)临时放置。收集数据以分析支架的技术成功率和临床转归(根据再发吞咽困难、并发症和再次干预评估)。
所有患者的支架植入均获得技术成功。11 例(11/30,36.7%)患者发生支架迁移,其中 SEPS 组 6 例(60%)、生物可降解支架组 2 例(20%)和 FCSEMS 组 3 例(30%)(P=0.16)。随访结束时,8/30 例(26.7%)患者无吞咽困难:SEPS 组 1 例(10%)、生物可降解支架组 3 例(30%)和 FCSEMS 组 4 例(40%)(P=0.27)。SEPS 组(n=24)再次干预的需求高于生物可降解支架组(n=13)和 FCSEMS 组(n=13)(P=0.24)。多变量分析显示,狭窄长度与临时支架置入后较高的复发率显著相关(HR=1.37;95%CI=1.08-1.75;P=0.011)。
在 RBES 患者中,临时放置生物可降解支架或 FCSEMS 可能分别导致 30%和 40%患者长期吞咽困难缓解。SEPS 似乎最不理想,因为其与支架频繁迁移、更多再次干预和较少长期改善相关。此外,较长的狭窄与更高的复发风险相关。