Warschkow Rene, Tarantino Ignazio, Lange Jochen, Müller Sascha A, Schmied Bruno M, Zünd Michael, Steffen Thomas
Department of Surgery, Kantonsspital St, Gallen (KSSG), St, Gallen, CH-9007, Switzerland.
Patient Saf Surg. 2012 Jun 15;6(1):12. doi: 10.1186/1754-9493-6-12.
For recurrent disease or primary therapy of advanced ovarian cancer, cytoreductive surgery (CRS) followed by adjuvant chemotherapy is a therapeutic option. The aim of this study was to evaluate the outcome for patients with epithelial ovarian cancer treated with hyperthermic intraoperative chemotherapy (HIPEC) and completeness of cytoreduction (CC).
Data were retrospectively collected from 111 patients with recurrent or primary ovarian cancer operated with the contribution of visceral surgical oncologists between 1991 and 2006 in a tertiary referral hospital.
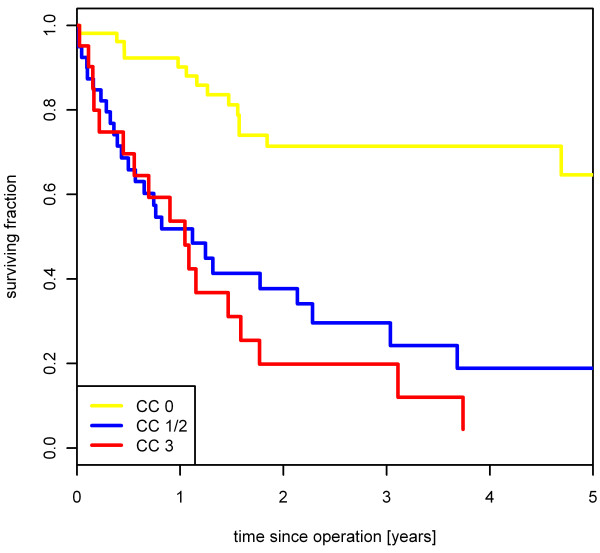
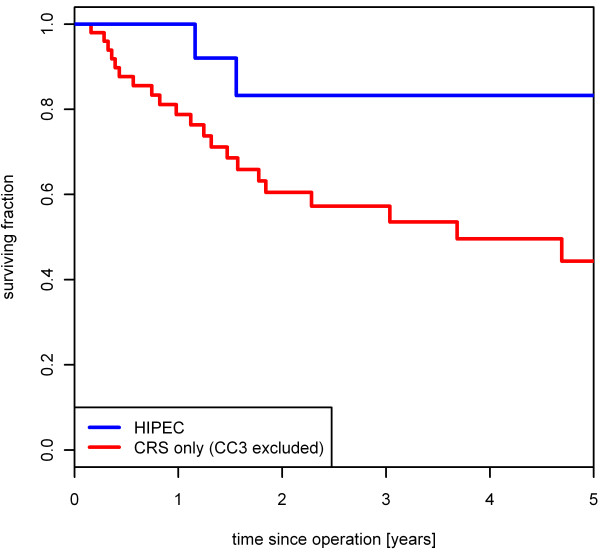
Ninety patients received CRS and 21 patients CRS plus HIPEC with cisplatin. Patients with complete cytoreduction (CC0) were more likely to receive HIPEC. Overall, 19 of 21 patients (90.5 %) with HIPEC and 33 of 90 patients (36.7 %) with CRS had a complete cytoreduction (P < 0.001). Incomplete cytoreduction was associated with worse survival rates with a hazard ratio (HR) of 4.4 (95%CI: 2.3-8.4) for CC1/2 and 6.0 (95%CI: 2.9-12.3) for CC3 (P < 0.001). In a Cox-regression limited to 52 patients with CC0 a systemic concomitant chemotherapy (HR 0.3, 95%CI: 0.1-0.96, P = 0.046) but not HIPEC (HR 0.98 with 95 % CI 0.32 to 2.97, P = 0.967) improved survival. Two patients (9.5 %) developed severe renal failure after HIPEC with absolute cisplatin dosages of 90 and 95 mg.
Completeness of cytoreduction was proved to be crucial for long-term outcome. HIPEC procedures in ovarian cancer should be performed in clinical trials to compare CRS, HIPEC and systemic chemotherapy against CRS with systemic chemotherapy. Concerning the safety of HIPEC with cisplatin, the risk of persistent renal failure must be considered when dosage is based on body surface.
对于复发性疾病或晚期卵巢癌的初始治疗,细胞减灭术(CRS)后辅助化疗是一种治疗选择。本研究的目的是评估接受术中热化疗(HIPEC)和细胞减灭完整性(CC)治疗的上皮性卵巢癌患者的预后。
回顾性收集了1991年至2006年间在一家三级转诊医院由内脏外科肿瘤学家参与手术的111例复发性或原发性卵巢癌患者的数据。
90例患者接受了CRS,21例患者接受了CRS加顺铂HIPEC。细胞减灭完全(CC0)的患者更有可能接受HIPEC。总体而言,21例接受HIPEC的患者中有19例(90.5%)实现了细胞减灭完全,90例接受CRS的患者中有33例(36.7%)实现了细胞减灭完全(P<0.001)。细胞减灭不完全与较差的生存率相关,CC1/2的风险比(HR)为4.4(95%CI:2.3-8.4),CC3的风险比为6.0(95%CI:2.9-12.3)(P<0.001)。在一项仅限于52例CC0患者的Cox回归分析中,全身同步化疗(HR 0.3,95%CI:0.1-0.96,P=0.046)而非HIPEC(HR 0.98,95%CI 0.32至2.97,P=0.967)可提高生存率。2例患者(9.5%)在接受绝对顺铂剂量分别为90和95mg的HIPEC后出现严重肾衰竭。
细胞减灭的完整性被证明对长期预后至关重要。卵巢癌的HIPEC手术应在临床试验中进行,以比较CRS、HIPEC和全身化疗与CRS加全身化疗的效果。关于顺铂HIPEC的安全性,当根据体表面积确定剂量时,必须考虑持续性肾衰竭的风险。