Kenya Medical Research Institute (KEMRI) Centre for Geographic Medicine Research - Coast, Nairobi, Kenya.
PLoS Med. 2012;9(6):e1001238. doi: 10.1371/journal.pmed.1001238. Epub 2012 Jun 12.
To improve care for children in district hospitals in Kenya, a multifaceted approach employing guidelines, training, supervision, feedback, and facilitation was developed, for brevity called the Emergency Triage and Treatment Plus (ETAT+) strategy. We assessed the cost effectiveness of the ETAT+ strategy, in Kenyan hospitals. Further, we estimate the costs of scaling up the intervention to Kenya nationally and potential cost effectiveness at scale.
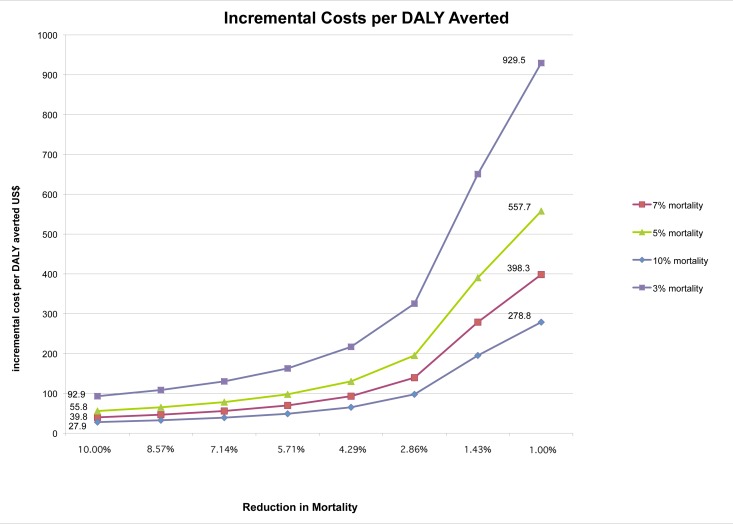
Our cost-effectiveness analysis from the provider's perspective used data from a previously reported cluster randomized trial comparing the full ETAT+ strategy (n = 4 hospitals) with a partial intervention (n = 4 hospitals). Effectiveness was measured using 14 process measures that capture improvements in quality of care; their average was used as a summary measure of quality. Economic costs of the development and implementation of the intervention were determined (2009 US$). Incremental cost-effectiveness ratios were defined as the incremental cost per percentage improvement in (average) quality of care. Probabilistic sensitivity analysis was used to assess uncertainty. The cost per child admission was US$50.74 (95% CI 49.26-67.06) in intervention hospitals compared to US$31.1 (95% CI 30.67-47.18) in control hospitals. Each percentage improvement in average quality of care cost an additional US$0.79 (95% CI 0.19-2.31) per admitted child. The estimated annual cost of nationally scaling up the full intervention was US$3.6 million, approximately 0.6% of the annual child health budget in Kenya. A "what-if" analysis assuming conservative reductions in mortality suggests the incremental cost per disability adjusted life year (DALY) averted by scaling up would vary between US$39.8 and US$398.3.
Improving quality of care at scale nationally with the full ETAT+ strategy may be affordable for low income countries such as Kenya. Resultant plausible reductions in hospital mortality suggest the intervention could be cost-effective when compared to incremental cost-effectiveness ratios of other priority child health interventions.
为了改善肯尼亚地区医院的儿童护理水平,我们采用了一种多方面的方法,包括制定指南、培训、监督、反馈和促进,简称为紧急分类和治疗加(ETAT+)策略。我们评估了 ETAT+策略在肯尼亚医院的成本效益。此外,我们还估算了在全国范围内推广该干预措施的成本以及在大规模推广时的潜在成本效益。
我们从提供者的角度进行的成本效益分析使用了先前报告的一项集群随机试验的数据,该试验比较了完整的 ETAT+策略(n=4 家医院)与部分干预(n=4 家医院)。使用 14 项过程指标来衡量护理质量的改善,这些指标的平均值被用作质量的综合衡量指标。确定了干预措施的开发和实施的经济成本(2009 年美元)。增量成本效益比定义为每提高(平均)护理质量的百分比所增加的成本。使用概率敏感性分析来评估不确定性。干预组每例入院患儿的费用为 50.74 美元(95%CI 49.26-67.06),对照组为 31.1 美元(95%CI 30.67-47.18)。每提高平均护理质量的 1%,每例入院患儿的额外成本为 0.79 美元(95%CI 0.19-2.31)。在全国范围内全面推广完整干预措施的年度成本估计为 360 万美元,约占肯尼亚儿童卫生年度预算的 0.6%。一项“假设分析”假设死亡率保守降低,表明通过扩大规模避免每例残疾调整生命年(DALY)的增量成本将在 39.8 美元至 398.3 美元之间变化。
在肯尼亚等低收入国家,全面实施 ETAT+策略以提高护理质量的规模可能是负担得起的。由于医院死亡率的降低幅度合理,该干预措施可能具有成本效益,与其他儿童健康干预措施的增量成本效益比相比。