Section of Neonatology, University of Manitoba, Winnipeg, MB, Canada.
BMC Pregnancy Childbirth. 2012 Jun 29;12:62. doi: 10.1186/1471-2393-12-62.
Infants born late preterm (34 + 0 to 36 + 6 weeks GA (gestational age)) are known to have higher neonatal morbidity than term (37 + 0 to 41 + 6 weeks GA) infants. There is emerging evidence that these risks may not be homogenous within the term cohort and may be higher in early term (37 + 0 to 38 + 6 weeks GA). These risks may also be affected by socioeconomic status, a risk factor for preterm birth.
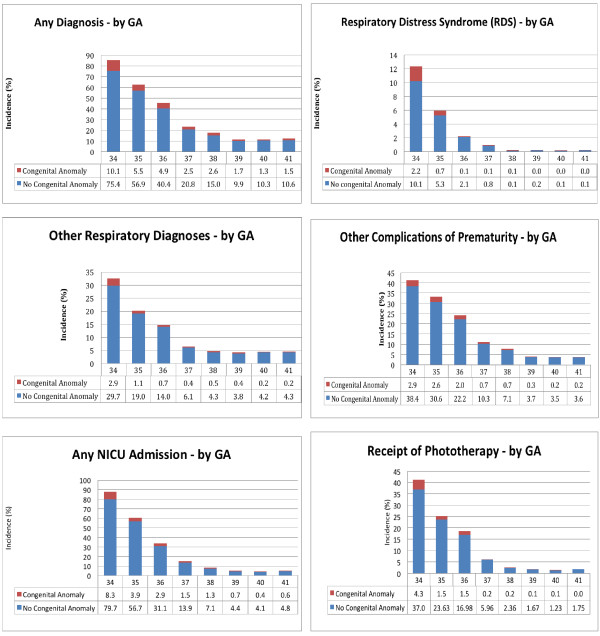
A retrospective population based cohort of infants born at 34 to 41 weeks of GA was assembled; individual and area-level income was used to develop three socioeconomic (SES) groups. Neonatal morbidity was grouped into respiratory distress syndrome (RDS), other respiratory disorders, other complications of prematurity, admission to a Level II/III nursery and receipt of phototherapy. Regression models were constructed to examine the relationship of GA and SES to neonatal morbidity while controlling for other perinatal variables.
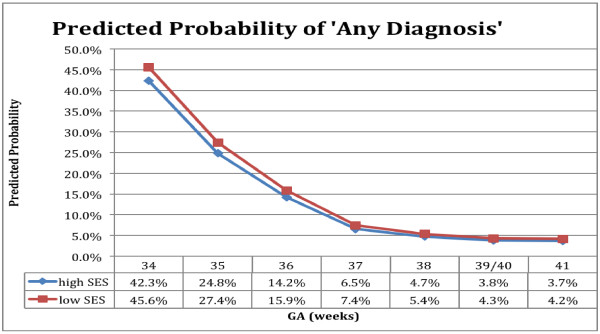
The cohort contained 25 312 infants of whom 6.1% (n = 1524) were born preterm and 32.4% (n = 8203) were of low SES. Using 39/40 weeks GA as the reference group there was a decrease in neonatal morbidity at each week of gestation. The odds ratios remained significantly higher at 37 weeks for RDS or other respiratory disorders, and at 38 weeks for all other outcomes. SES had an independent effect, increasing morbidity with odds ratios ranging from 1.2-1.5 for all outcomes except for the RDS group, where it was not significant.
The risks of morbidity fell throughout late preterm and early term gestation for both respiratory and non-respiratory morbidity. Low SES was associated with an independent increased risk. Recognition that the morbidities associated with prematurity continue into early term gestation and are further compounded by SES is important to develop strategies for improving care of early term infants, avoiding iatrogenic complications and prioritizing public health interventions.
相较于足月(37+0 至 41+6 周 GA)儿,晚早产儿(34+0 至 36+6 周 GA)出生后具有更高的新生儿发病率。目前有证据表明,这些风险在足月儿中并非同质的,并且在早期足月(37+0 至 38+6 周 GA)儿中风险更高。这些风险也可能受到社会经济地位(早产的一个危险因素)的影响。
我们组建了一个基于人群的回顾性队列,纳入了在 34 至 41 周 GA 出生的婴儿;个体和地区收入被用来划分三个社会经济(SES)群体。新生儿发病率被分为呼吸窘迫综合征(RDS)、其他呼吸系统疾病、早产儿其他并发症、入住二级/三级新生儿监护室和接受光疗。构建回归模型,在控制其他围产期变量的情况下,研究 GA 和 SES 与新生儿发病率的关系。
该队列包含 25312 名婴儿,其中 6.1%(n=1524)为早产儿,32.4%(n=8203)SES 较低。以 39/40 周 GA 为参照组,每增加一周妊娠,新生儿发病率均降低。37 周时 RDS 或其他呼吸系统疾病的比值比仍显著升高,38 周时所有其他结局的比值比也显著升高。SES 有独立影响,除 RDS 组外,所有结局的发病率比值比均为 1.2-1.5,而在 RDS 组中,这种关联不显著。
晚早产儿和早期足月儿的呼吸系统和非呼吸系统发病率在整个孕期均有所下降。SES 较低与发病率的独立增加风险相关。认识到与早产相关的发病率持续到早期足月妊娠,并且 SES 进一步加重了这种情况,对于制定改善早期足月儿护理、避免医源性并发症和优先实施公共卫生干预的策略非常重要。