Department of Psychiatry & Behavioral Sciences, Stanford University School of Medicine, Stanford, California 94305–5722, USA.
Depress Anxiety. 2012 Oct;29(10):896-905. doi: 10.1002/da.21977. Epub 2012 Jul 5.
Findings regarding the relationship between patient treatment preference and treatment outcome are mixed. This is a secondary data analysis investigating the relationship between treatment preference, and symptom outcome and attrition in a large two-phase depression treatment trial.
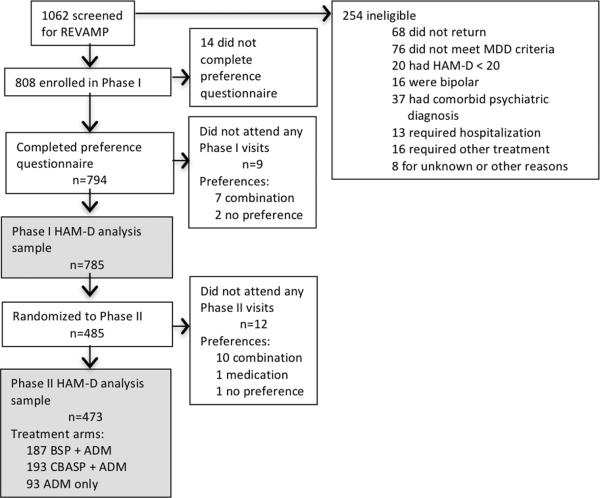
Patients met DSM-IV criteria for chronic forms of depression. Phase I was a 12-week, nonrandomized, open-label trial in which all participants (n = 785) received antidepressant medication(s) (ADM). Phase I nonremitters were randomized to Phase II, in which they received 12 weeks of either cognitive-behavioral system of psychotherapy (CBASP) + ADM (n = 193), brief supportive psychotherapy (BSP) + ADM (n = 187), or ADM only (n = 93). Participants indicated their treatment preference (medication only, combined treatment or no preference) at study entry. Symptoms were measured at 2-week intervals with the 24-item Hamilton Rating Scale for Depression (HAM-D).
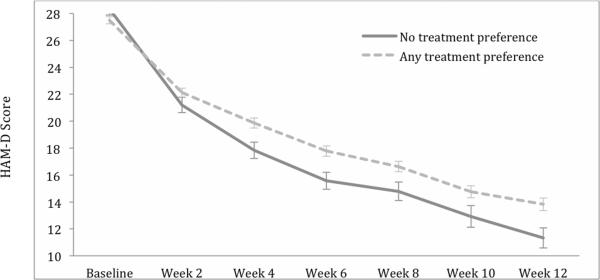
A large majority of patients reported a preference for combined treatment. Patients who preferred medication only were more likely to endorse a chemical imbalance explanation for depression, whereas those desiring combined treatment were more likely to attribute their depression to stressful experiences. In Phase I, patients who expressed no treatment preference showed greater rates of HAM-D symptom reduction than those with any preference, and patients with a preference for medication showed higher attrition than those preferring combined treatment. In Phase II, baseline treatment preference was not associated with symptom reduction or attrition.
Treatment preferences may moderate treatment response and attrition in unexpected ways. Research identifying factors associated with differing preferences may enable improved treatment retention and response.
关于患者治疗偏好与治疗结果之间关系的研究结果不一。本研究是一项二次数据分析,旨在探讨一项大型双相抑郁治疗试验中治疗偏好与症状结果和脱落之间的关系。
患者符合 DSM-IV 慢性抑郁标准。第 I 阶段为 12 周的非随机、开放性试验,所有参与者(n=785)均接受抗抑郁药物(ADM)治疗。第 I 阶段未缓解者被随机分配到第 II 阶段,他们接受 12 周的认知行为系统心理治疗(CBASP+ADM,n=193)、简短支持性心理治疗(BSP+ADM,n=187)或仅 ADM(n=93)治疗。参与者在研究入组时表明其治疗偏好(仅药物、联合治疗或无偏好)。使用 24 项汉密尔顿抑郁量表(HAM-D)每隔 2 周测量症状。
绝大多数患者报告了对联合治疗的偏好。仅选择药物治疗的患者更有可能认同抑郁症是化学失衡的解释,而那些希望联合治疗的患者更有可能将其抑郁症归因于压力经历。在第 I 阶段,未表达治疗偏好的患者比有任何偏好的患者HAM-D 症状减轻率更高,而选择药物治疗的患者比选择联合治疗的患者脱落率更高。在第 II 阶段,基线治疗偏好与症状减轻或脱落无关。
治疗偏好可能以意想不到的方式调节治疗反应和脱落。研究确定与不同偏好相关的因素可能有助于提高治疗保留率和反应率。