Harborview Medical Center, Division of Pulmonary and Critical Care, Department of Medicine, University of Washington, Seattle, WA, USA.
Contemp Clin Trials. 2012 Nov;33(6):1245-54. doi: 10.1016/j.cct.2012.06.010. Epub 2012 Jul 6.
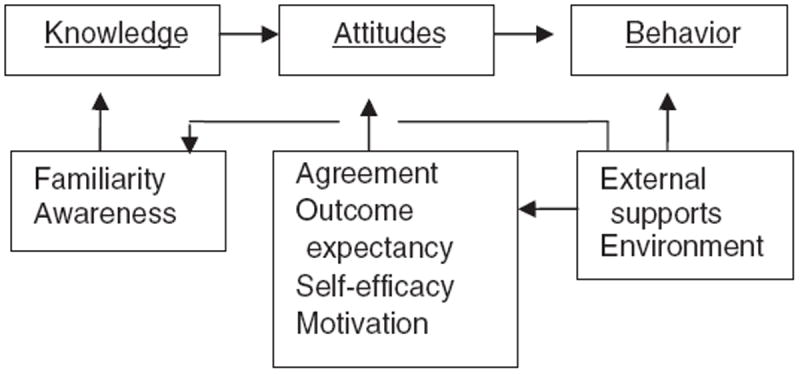
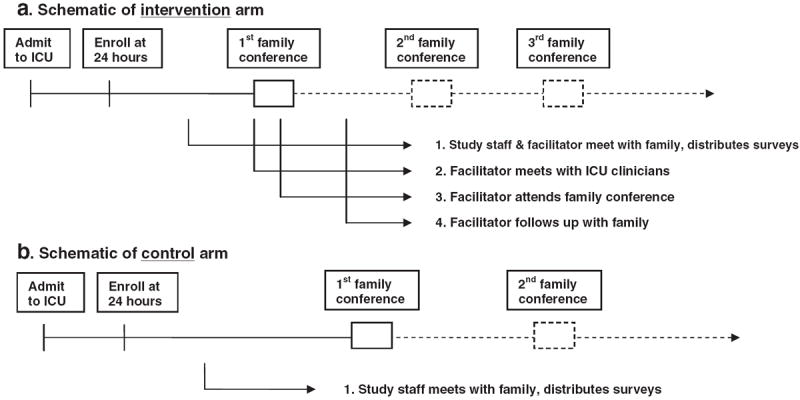
The intensive care unit (ICU), where death is common and even survivors of an ICU stay face the risk of long-term morbidity and re-admissions to the ICU, represents an important setting for improving communication about palliative and end-of-life care. Communication about the goals of care in this setting should be a high priority since studies suggest that the current quality of ICU communication is often poor and is associated with psychological distress among family members of critically ill patients. This paper describes the development and evaluation of an intervention designed to improve the quality of care in the ICU by improving communication among the ICU team and with family members of critically ill patients. We developed a multi-faceted, interprofessional intervention based on self-efficacy theory. The intervention involves a "communication facilitator" - a nurse or social worker - trained to facilitate communication among the interprofessional ICU team and with the critically ill patient's family. The facilitators are trained using three specific content areas: a) evidence-based approaches to improving clinician-family communication in the ICU, b) attachment theory allowing clinicians to adapt communication to meet individual family member's communication needs, and c) mediation to facilitate identification and resolution of conflict including clinician-family, clinician-clinician, and intra-family conflict. The outcomes assessed in this randomized trial focus on psychological distress among family members including anxiety, depression, and post-traumatic stress disorder at 3 and 6 months after the ICU stay. This manuscript also reports some of the lessons that we have learned early in this study.
重症监护病房(ICU)是死亡常见的地方,即使是 ICU 幸存者也面临长期发病和再次入住 ICU 的风险,因此这是一个改善姑息治疗和临终关怀沟通的重要场所。由于研究表明,目前 ICU 沟通的质量往往较差,并且与重症患者家属的心理困扰有关,因此在该环境中讨论护理目标应是重中之重。本文介绍了一种干预措施的开发和评估情况,该干预措施旨在通过改善 ICU 团队内部以及与重症患者家属之间的沟通来提高 ICU 的护理质量。我们根据自我效能理论开发了一种多方面的、多专业的干预措施。该干预措施涉及到一名“沟通促进者”——一名受过培训的护士或社会工作者,以促进跨专业 ICU 团队之间以及与重症患者家属之间的沟通。促进者接受了三个特定内容领域的培训:a)改善 ICU 中临床医生与家属沟通的循证方法;b)依恋理论,使临床医生能够根据个人家属的沟通需求调整沟通方式;c)调解,以促进识别和解决冲突,包括临床医生与家属之间、临床医生与临床医生之间以及家庭内部的冲突。本随机试验评估的结果主要集中在 ICU 后 3 个月和 6 个月时家属的心理困扰,包括焦虑、抑郁和创伤后应激障碍。本文还报告了我们在研究早期学到的一些经验教训。