Department of Radiology, Johns Hopkins University School of Medicine, Baltimore, Maryland, United States of America.
PLoS One. 2012;7(7):e41974. doi: 10.1371/journal.pone.0041974. Epub 2012 Jul 30.
To quantify resting myocardial blood flow (MBF) in the left ventricular (LV) wall of HCM patients and to determine the relationship to important parameters of disease: LV wall thickness, late gadolinium enhancement (LGE), T2-signal abnormalities (dark and bright signal), LV outflow tract obstruction and age.
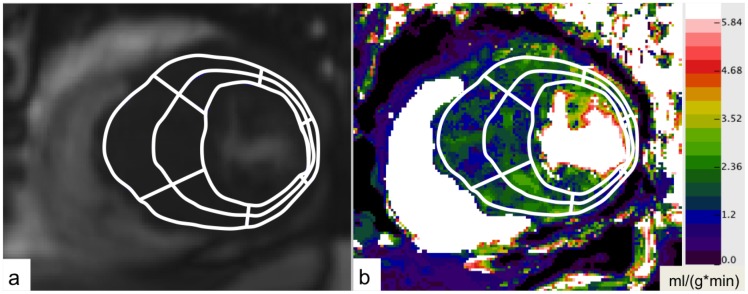
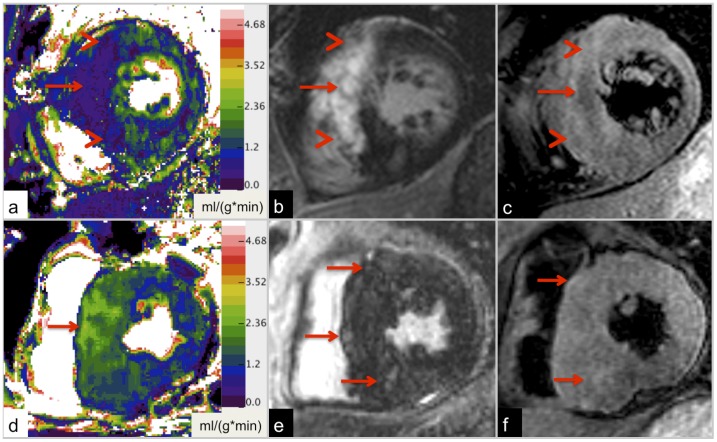
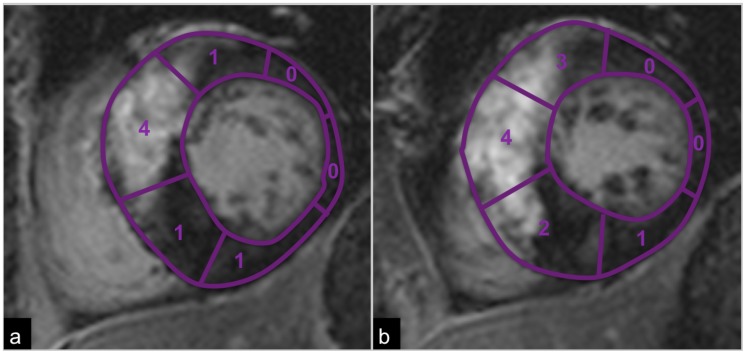
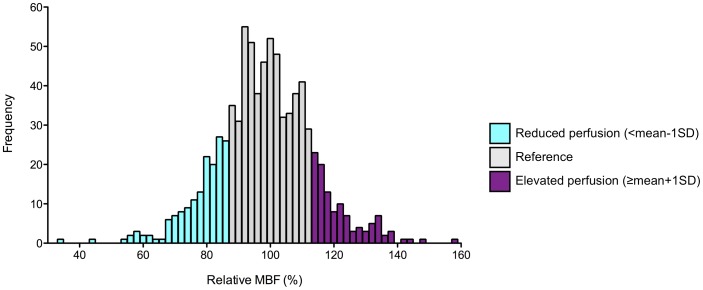
Seventy patients with proven HCM underwent cardiac MRI. Absolute and relative resting MBF were calculated from cardiac perfusion MRI by using the Fermi function model. The relationship between relative MBF and LV wall thickness, T2-signal abnormalities (T2 dark and T2 bright signal), LGE, age and LV outflow gradient as determined by echocardiography was determined using simple and multiple linear regression analysis. Categories of reduced and elevated perfusion in relation to non- or mildly affected reference segments were defined, and T2-signal characteristics and extent as well as pattern of LGE were examined. Statistical testing included linear and logistic regression analysis, unpaired t-test, odds ratios, and Fisher's exact test.
804 segments in 70 patients were included in the analysis. In a simple linear regression model LV wall thickness (p<0.001), extent of LGE (p<0.001), presence of edema, defined as focal T2 bright signal (p<0.001), T2 dark signal (p<0.001) and age (p = 0.032) correlated inversely with relative resting MBF. The LV outflow gradient did not show any effect on resting perfusion (p = 0.901). Multiple linear regression analysis revealed that LGE (p<0.001), edema (p = 0.026) and T2 dark signal (p = 0.019) were independent predictors of relative resting MBF. Segments with reduced resting perfusion demonstrated different LGE patterns compared to segments with elevated resting perfusion.
In HCM resting MBF is significantly reduced depending on LV wall thickness, extent of LGE, focal T2 signal abnormalities and age. Furthermore, different patterns of perfusion in HCM patients have been defined, which may represent different stages of disease.
定量肥厚型心肌病(HCM)患者左心室(LV)壁的静息心肌血流(MBF),并确定与疾病的重要参数之间的关系:LV 壁厚度、晚期钆增强(LGE)、T2 信号异常(暗信号和亮信号)、LV 流出道梗阻和年龄。
70 例经证实的 HCM 患者接受心脏 MRI 检查。通过使用费米函数模型从心脏灌注 MRI 计算绝对和相对静息 MBF。使用简单和多元线性回归分析确定相对 MBF 与 LV 壁厚度、T2 信号异常(T2 暗信号和 T2 亮信号)、LGE、年龄以及超声心动图确定的 LV 流出梯度之间的关系。根据非受累或轻度受累参考节段定义灌注减少和增加的类别,并检查 T2 信号特征和程度以及 LGE 的模式。统计检验包括线性和逻辑回归分析、配对 t 检验、优势比和 Fisher 精确检验。
70 例患者的 804 个节段纳入分析。在简单线性回归模型中,LV 壁厚度(p<0.001)、LGE 程度(p<0.001)、存在水肿,定义为局灶性 T2 亮信号(p<0.001)、T2 暗信号(p<0.001)和年龄(p=0.032)与相对静息 MBF 呈负相关。LV 流出梯度对静息灌注没有任何影响(p=0.901)。多元线性回归分析显示,LGE(p<0.001)、水肿(p=0.026)和 T2 暗信号(p=0.019)是相对静息 MBF 的独立预测因子。与静息灌注增加的节段相比,静息灌注减少的节段显示出不同的 LGE 模式。
在 HCM 中,静息 MBF 显著降低,取决于 LV 壁厚度、LGE 程度、局灶性 T2 信号异常和年龄。此外,已经定义了 HCM 患者不同的灌注模式,这可能代表了不同的疾病阶段。