Primary Healthcare Research Unit, Memorial University of Newfoundland, Health Sciences Centre, St, John's, Newfoundland and Labrador, St Johns, Canada.
BMC Emerg Med. 2012 Aug 14;12:11. doi: 10.1186/1471-227X-12-11.
Rupture of the spleen in the absence of trauma or previously diagnosed disease is largely ignored in the emergency literature and is often not documented as such in journals from other fields. We have conducted a systematic review of the literature to highlight the surprisingly frequent occurrence of this phenomenon and to document the diversity of diseases that can present in this fashion.
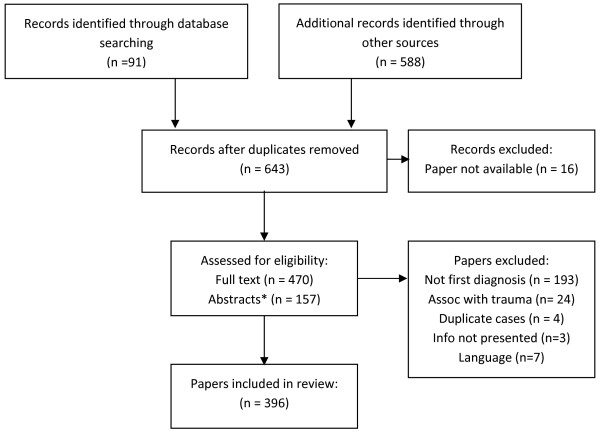
Systematic review of English and French language publications catalogued in Pubmed, Embase and CINAHL between 1950 and 2011.
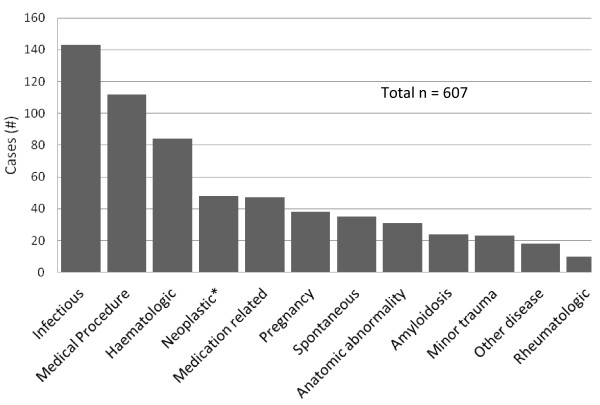
We found 613 cases of splenic rupture meeting the criteria above, 327 of which occurred as the presenting complaint of an underlying disease and 112 of which occurred following a medical procedure. Rupture appeared to occur spontaneously in histologically normal (but not necessarily normal size) spleens in 35 cases and after minor trauma in 23 cases. Medications were implicated in 47 cases, a splenic or adjacent anatomical abnormality in 31 cases and pregnancy or its complications in 38 cases. The most common associated diseases were infectious (n = 143), haematologic (n = 84) and non-haematologic neoplasms (n = 48). Amyloidosis (n = 24), internal trauma such as cough or vomiting (n = 17) and rheumatologic diseases (n = 10) are less frequently reported. Colonoscopy (n = 87) was the procedure reported most frequently as a cause of rupture. The anatomic abnormalities associated with rupture include splenic cysts (n = 6), infarction (n = 6) and hamartomata (n = 5). Medications associated with rupture include anticoagulants (n = 21), thrombolytics (n = 13) and recombinant G-CSF (n = 10). Other causes or associations reported very infrequently include other endoscopy, pulmonary, cardiac or abdominal surgery, hysterectomy, peliosis, empyema, remote pancreato-renal transplant, thrombosed splenic vein, hemangiomata, pancreatic pseudocysts, splenic artery aneurysm, cholesterol embolism, splenic granuloma, congenital diaphragmatic hernia, rib exostosis, pancreatitis, Gaucher's disease, Wilson's disease, pheochromocytoma, afibrinogenemia and ruptured ectopic pregnancy.
Emergency physicians should be attuned to the fact that rupture of the spleen can occur in the absence of major trauma or previously diagnosed splenic disease. The occurrence of such a rupture is likely to be the manifesting complaint of an underlying disease. Furthermore, colonoscopy should be more widely documented as a cause of splenic rupture.
在急诊文献中,脾脏破裂而无外伤或先前诊断的疾病在很大程度上被忽视,而且在其他领域的期刊中也往往没有记录。我们对文献进行了系统回顾,以强调这种现象的发生频率之高,并记录可能以这种方式出现的各种疾病。
对 1950 年至 2011 年期间在 Pubmed、Embase 和 CINAHL 中编目的英语和法语出版物进行系统回顾。
我们发现了 613 例符合上述标准的脾破裂病例,其中 327 例为基础疾病的首发表现,112 例发生在医疗程序后。脾破裂似乎在组织学正常(但不一定正常大小)的脾脏中自发性发生,35 例脾破裂后发生轻微外伤,23 例脾破裂后发生轻微外伤。47 例与药物有关,31 例与脾脏或相邻解剖异常有关,38 例与妊娠或其并发症有关。最常见的相关疾病为感染性疾病(n=143)、血液系统疾病(n=84)和非血液系统肿瘤(n=48)。淀粉样变性(n=24)、咳嗽或呕吐等内部创伤(n=17)和风湿性疾病(n=10)较少见。结直肠镜检查(n=87)是报告最频繁的破裂原因。与破裂相关的解剖异常包括脾囊肿(n=6)、梗死(n=6)和错构瘤(n=5)。与破裂相关的药物包括抗凝剂(n=21)、溶栓剂(n=13)和重组 G-CSF(n=10)。其他非常少见的原因或关联包括其他内镜、肺、心脏或腹部手术、子宫切除术、血窦、脓胸、远端胰腺-肾移植、脾静脉血栓形成、血管瘤、胰腺假性囊肿、脾动脉动脉瘤、胆固醇栓塞、脾肉芽肿、先天性膈疝、肋骨外生骨疣、胰腺炎、戈谢病、威尔逊病、嗜铬细胞瘤、无纤维蛋白原血症和破裂的异位妊娠。
急诊医师应注意到,脾脏破裂可发生于无重大外伤或先前诊断的脾脏疾病的情况下。这种破裂的发生很可能是潜在疾病的表现。此外,结直肠镜检查应更广泛地记录为脾破裂的原因。