Medical Intensive Care Unit, University Hospitals Leuven, Leuven, Belgium.
Intensive Care Med. 2012 Nov;38(11):1761-8. doi: 10.1007/s00134-012-2673-2. Epub 2012 Aug 16.
Despite their controversial role, corticosteroids (CS) are frequently administered to patients with H1N1 virus infection with severe respiratory failure secondary to viral pneumonia. We hypothesized that invasive pulmonary aspergillosis (IPA) is a frequent complication in critically ill patients with H1N1 virus infection and that CS may contribute to this complication.
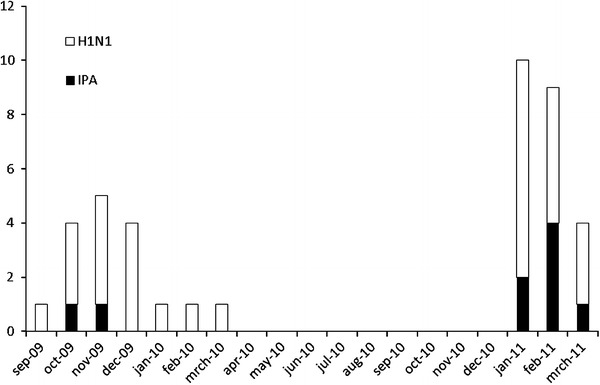
We retrospectively selected all adult patients with confirmed H1N1 virus infection admitted to the intensive care unit (ICU) of two tertiary care hospitals from September 2009 to March 2011. Differences in baseline factors, risk factors, and outcome parameters were studied between patients with and without IPA.
Of 40 critically ill patients with confirmed H1N1, 9 (23 %) developed IPA 3 days after ICU admission. Five patients had proven and four had probable IPA. Significantly more IPA patients received CS within 7 days before ICU admission (78 versus 23 %, p = 0.002). IPA patients also received significantly higher doses of CS before ICU admission [hydrocortisone equivalent 800 (360-2,635) versus 0 (0-0) mg, p = 0.005]. On multivariate analysis, use of CS before ICU admission was independently associated with IPA [odds ratio (OR) 14.4 (2.0-101.6), p = 0.007].
IPA was diagnosed in 23 % of critically ill patients with H1N1 virus infection after a median of 3 days after ICU admission. Our data suggest that use of CS 7 days before ICU admission is an independent risk factor for fungal superinfection. These findings may have consequences for clinical practice as they point out the need for increased awareness of IPA, especially in those critically ill H1N1 patients already receiving CS.
尽管皮质类固醇(CS)存在争议,但对于因病毒性肺炎继发严重呼吸衰竭而导致 H1N1 病毒感染的患者,仍常给予 CS 治疗。我们假设,侵袭性肺曲霉病(IPA)是重症 H1N1 病毒感染患者的常见并发症,CS 可能导致这一并发症。
我们回顾性选择了 2009 年 9 月至 2011 年 3 月期间入住两家三级医院重症监护病房(ICU)的所有成人确诊 H1N1 病毒感染患者。研究了有和无 IPA 患者之间的基线因素、危险因素和预后参数差异。
在 40 例确诊的 H1N1 危重症患者中,9 例(23%)在 ICU 入住后 3 天发生 IPA。5 例为确诊 IPA,4 例为可能 IPA。入住 ICU 前 7 天内,IPA 患者更常接受 CS 治疗(78%比 23%,p=0.002)。IPA 患者在入住 ICU 前接受的 CS 剂量也明显更高[等效氢化可的松剂量 800(360-2635)比 0(0-0)mg,p=0.005]。多变量分析显示,入住 ICU 前使用 CS 与 IPA 独立相关[比值比(OR)14.4(2.0-101.6),p=0.007]。
在 ICU 入住后中位数 3 天,诊断出 23%的 H1N1 病毒感染危重症患者发生 IPA。我们的数据表明,入住 ICU 前 7 天使用 CS 是真菌感染的独立危险因素。这些发现可能对临床实践产生影响,因为它们指出了需要提高对 IPA 的认识,尤其是在已经接受 CS 治疗的危重 H1N1 患者中。