Yale Global Health Leadership Institute, Yale School of Public Health, 60 College Street, PO Box 208034, New Haven, CT, USA.
Hum Resour Health. 2012 Sep 13;10:33. doi: 10.1186/1478-4491-10-33.
Leadership is widely regarded as central to effective health-care systems, and resources are increasingly devoted to the cultivation of strong health-care leadership. Nevertheless, the literature regarding leadership capacity building has been developed primarily in the context of high-income settings. Less research has been done on leadership in low-income settings, including sub-Saharan Africa, particularly in health care, with attention to historical, political and sociocultural context. We sought to characterize the experiences of individuals in key health-care leadership roles in sub-Saharan Africa.
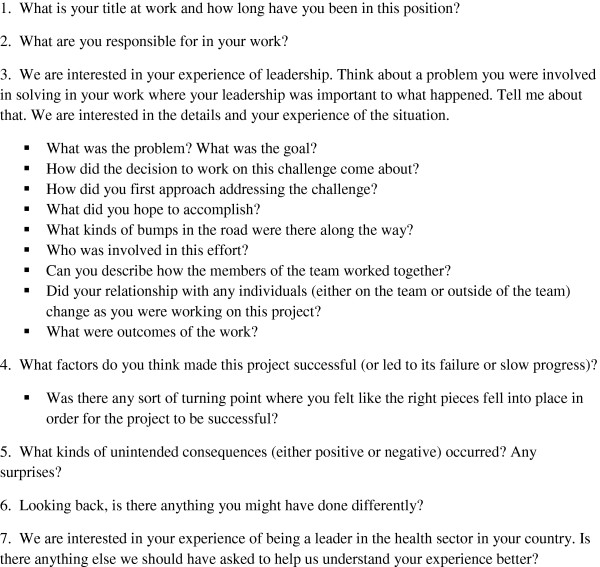
We conducted a qualitative study using in-person interviews with individuals (n = 17) in health-care leadership roles in four countries in sub-Saharan Africa: the Federal Democratic Republic of Ethiopia, the Republic of Ghana, the Republic of Liberia and the Republic of Rwanda. Individuals were identified by their country's minister of health as key leaders in the health sector and were nominated to serve as delegates to a global health leadership conference in June 2010, at Yale University in the United States. Interviews were audio recorded and professionally transcribed. Data analysis was performed by a five-person multidisciplinary team using the constant comparative method, facilitated by ATLAS.ti 5.0 software.
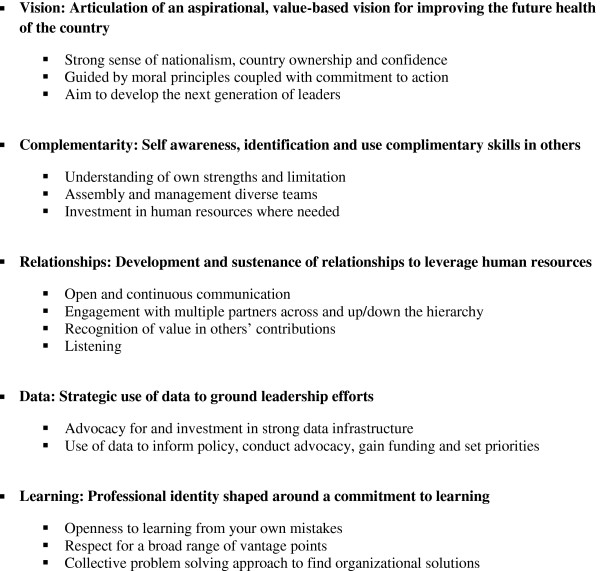
Five key themes emerged as important to participants in their leadership roles: having an aspirational, value-based vision for improving the future health of the country, being self-aware and having the ability to identify and use complementary skills of others, tending to relationships, using data in decision making, and sustaining a commitment to learning.
Current models of leadership capacity building address the need for core technical and management competencies. While these competencies are important, skills relevant to managing relationships are also critical in the sub-Saharan African context. Developing such skills may require more time and a deeper level of engagement and collaboration than is typically invested in efforts to strengthen health systems.
领导力被广泛认为是有效医疗体系的核心,越来越多的资源被投入到培养强大的医疗领导力中。然而,关于领导力能力建设的文献主要是在高收入环境下发展起来的。在包括撒哈拉以南非洲在内的低收入环境中,对领导力的研究较少,尤其是在医疗保健方面,关注的是历史、政治和社会文化背景。我们试图描述撒哈拉以南非洲关键医疗保健领导角色中的个人的经验。
我们采用定性研究方法,对来自撒哈拉以南非洲四个国家(埃塞俄比亚联邦民主共和国、加纳共和国、利比里亚共和国和卢旺达共和国)医疗保健领导角色的 17 名个人(n=17)进行了面对面访谈。这些个人是由各自国家的卫生部长确定为卫生部门的主要领导人,并被提名作为代表参加 2010 年 6 月在美国耶鲁大学举行的全球卫生领导力会议。访谈内容进行了录音,并由专业人员进行了转录。由五名跨学科人员组成的团队使用恒定比较法进行数据分析,使用 ATLAS.ti 5.0 软件进行辅助。
五个关键主题在参与者的领导角色中被认为是重要的:对改善国家未来健康状况有一个有抱负的、基于价值观的愿景,具有自我意识,并有能力识别和利用他人的互补技能,关注人际关系,在决策中使用数据,并坚持学习的承诺。
当前的领导力能力建设模式满足了对核心技术和管理能力的需求。虽然这些能力很重要,但在撒哈拉以南非洲背景下,管理关系的相关技能也至关重要。培养这些技能可能需要比加强卫生系统的努力投入更多的时间和更深入的参与和合作。