Jung Yun Jung, Chung Wou Young, Lee Miyeon, Lee Keu Sung, Park Joo Hun, Sheen Seung Soo, Hwang Sung Chul, Park Kwang Joo
Department of Pulmonary and Critical Care Medicine, Ajou University School of Medicine, Suwon, Korea.
Tuberc Respir Dis (Seoul). 2012 Sep;73(3):151-61. doi: 10.4046/trd.2012.73.3.151. Epub 2012 Sep 28.
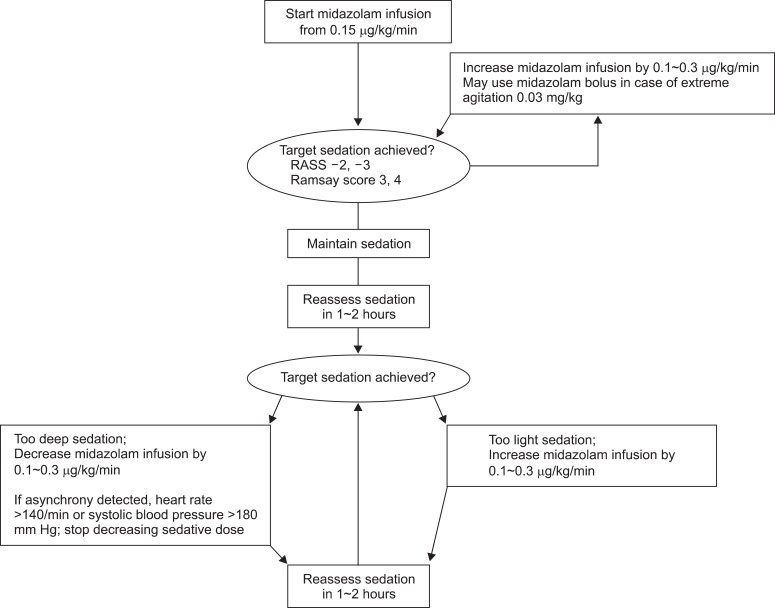
Adequate assessment and control of sedation play crucial roles in the proper performance of mechanical ventilation.
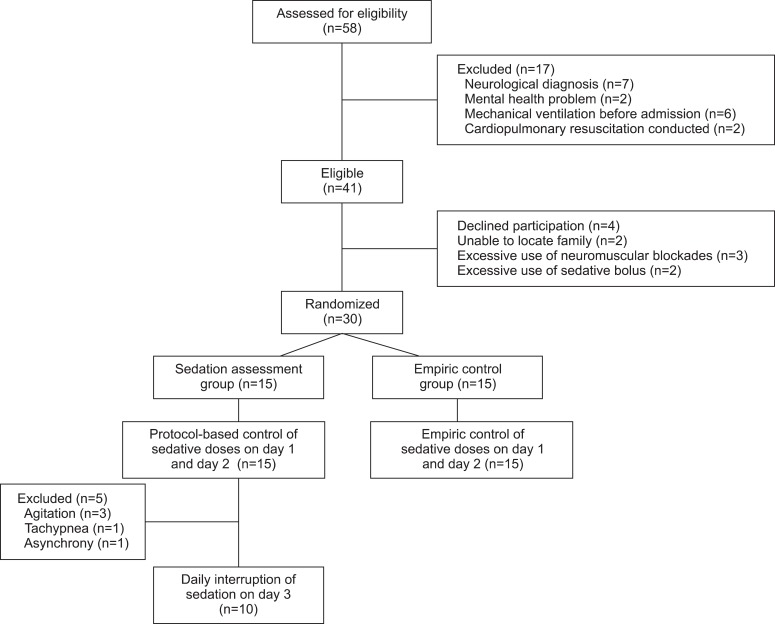
A total of 30 patients with various pulmonary diseases were prospectively enrolled. The study population was randomized into two groups. The sedation assessment group (SAG) received active protocol-based control of sedation, and in the empiric control group (ECG), the sedation levels were empirically adjusted. Subsequently, daily interruption of sedation (DIS) was conducted in the SAG.
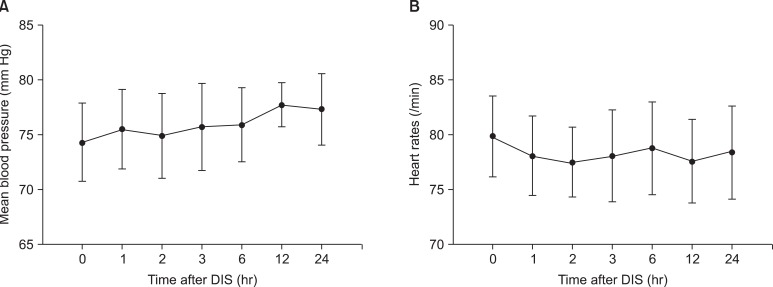
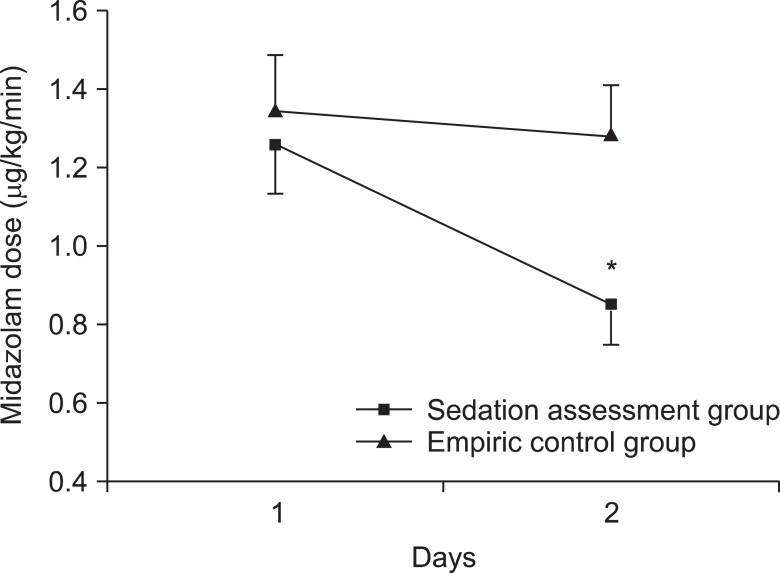
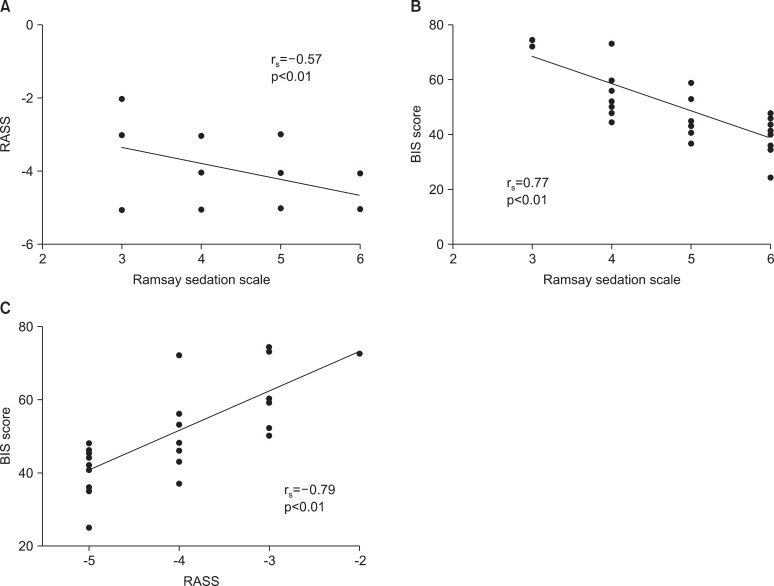
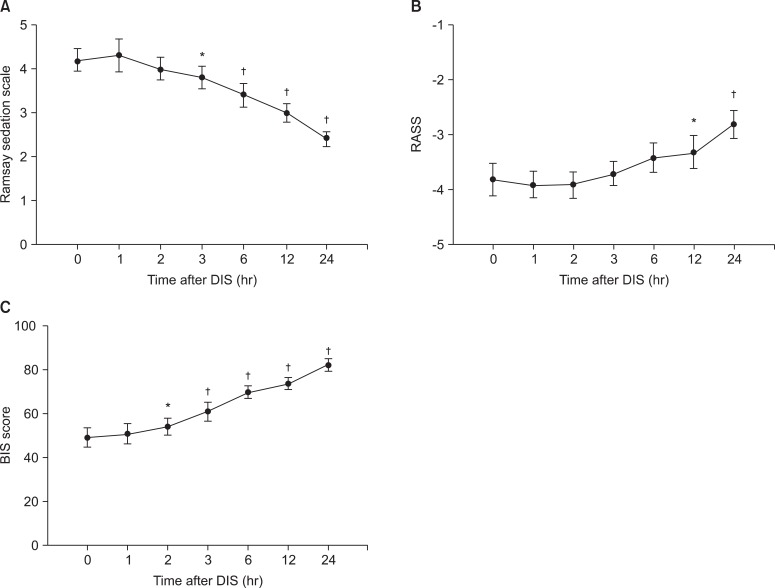
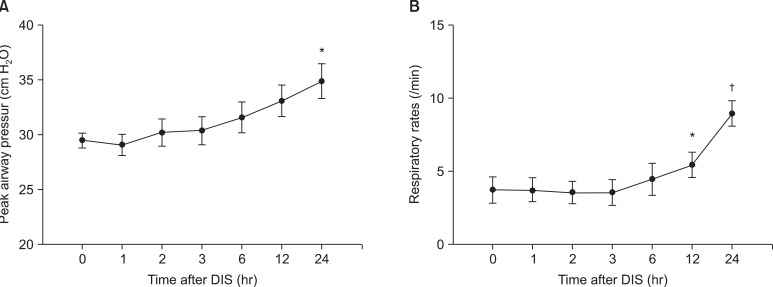
In the SAG, the dose of midazolam was significantly reduced by control of sedation (day 1, 1.3±0.5 µg/kg/min; day 2, 0.9±0.4 µg/kg/min; p<0.01), and was significantly lower than the ECG on day 2 (p<0.01). Likewise, on day 2, sedation levels were significantly lower in the SAG than in the ECG. Significant relationship was found between Ramsay sedation scale and Richmond agitation-sedation scale (RASS; r(s)=-0.57), Ramsay Sedation Scale and Bispectral Index (BIS; r(s)=0.77), and RASS and BIS (r(s)=-0.79). In 10 patients, who didn't require re-sedation after DIS, BIS showed the earliest and most significant changes among the sedation scales. Ventilatory parameters showed significant but less prominent changes, and hemodynamic parameters didn't show significant changes. No seriously adverse events ensued after the implementation of DIS.
Active assessment and control of sedation significantly reduced the dosage of sedatives in patients receiving mechanical ventilation. DIS, conducted in limited cases, suggested its potential efficacy and tolerability.
充分评估和控制镇静在机械通气的正确实施中起着关键作用。
前瞻性纳入30例患有各种肺部疾病的患者。研究人群被随机分为两组。镇静评估组(SAG)接受基于方案的积极镇静控制,而经验性控制组(ECG)则根据经验调整镇静水平。随后,在SAG组中进行每日镇静中断(DIS)。
在SAG组中,通过镇静控制,咪达唑仑的剂量显著降低(第1天,1.3±0.5μg/kg/min;第2天,0.9±0.4μg/kg/min;p<0.01),且在第2天显著低于ECG组(p<0.01)。同样,在第2天,SAG组的镇静水平显著低于ECG组。Ramsay镇静评分与Richmond躁动-镇静评分(RASS)之间存在显著相关性(r(s)=-0.57),Ramsay镇静评分与脑电双频指数(BIS)之间存在显著相关性(r(s)=0.77),RASS与BIS之间存在显著相关性(r(s)=-0.79)。在10例DIS后无需重新镇静的患者中,BIS在所有镇静评分中显示出最早且最显著的变化。通气参数有显著但不太明显的变化,但血流动力学参数无显著变化。实施DIS后未发生严重不良事件。
积极评估和控制镇静可显著降低接受机械通气患者的镇静剂用量。在有限病例中进行的DIS表明了其潜在的疗效和耐受性。