Department of Primary and Community Care, Radboud University Nijmegen Medical Centre, P O Box 9101, 6500 HB Nijmegen, Netherlands.
BMJ. 2012 Nov 28;345:e7642. doi: 10.1136/bmj.e7642.
To assess the long term effects of two different modes of disease management (comprehensive self management and routine monitoring) on quality of life (primary objective), frequency and patients' management of exacerbations, and self efficacy (secondary objectives) in patients with chronic obstructive pulmonary disease (COPD) in general practice.
24 month, multicentre, investigator blinded, three arm, pragmatic, randomised controlled trial.
15 general practices in the eastern part of the Netherlands.
Patients with COPD confirmed by spirometry and treated in general practice. Patients with very severe COPD or treated by a respiratory physician were excluded.
A comprehensive self management programme as an adjunct to usual care, consisting of four tailored sessions with ongoing telephone support by a practice nurse; routine monitoring as an adjunct to usual care, consisting of 2-4 structured consultations a year with a practice nurse; or usual care alone (contacts with the general practitioner at the patients' own initiative).
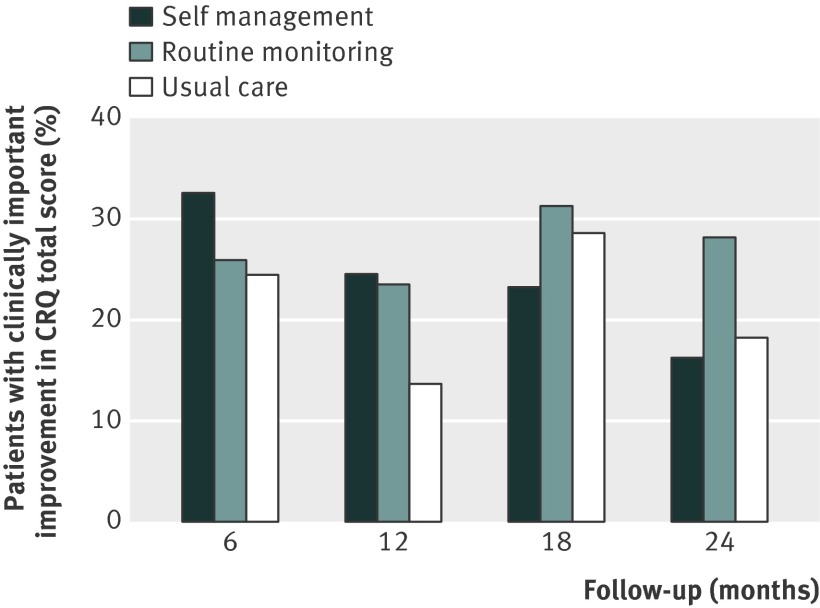
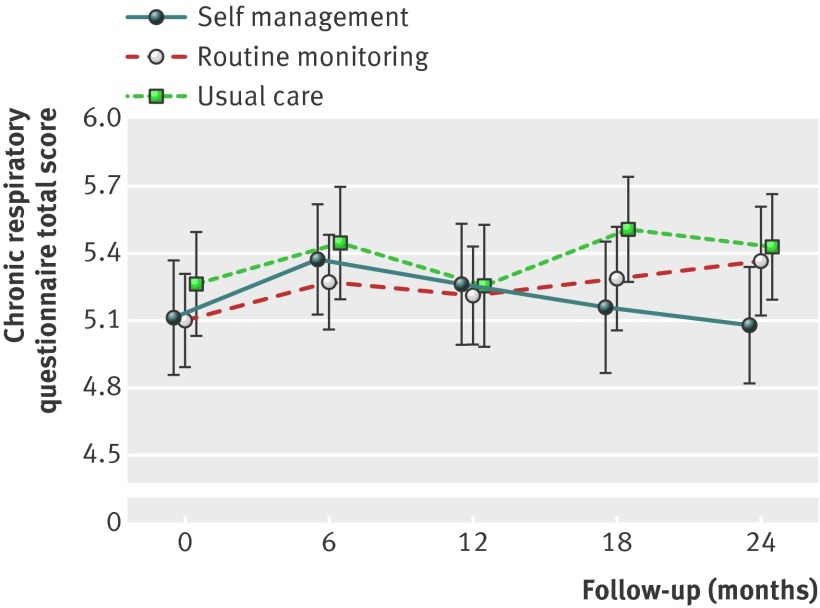
The primary outcome was the change in COPD specific quality of life at 24 months as measured with the chronic respiratory questionnaire total score. Secondary outcomes were chronic respiratory questionnaire domain scores, frequency and patients' management of exacerbations measured with the Nijmegen telephonic exacerbation assessment system, and self efficacy measured with the COPD self-efficacy scale.
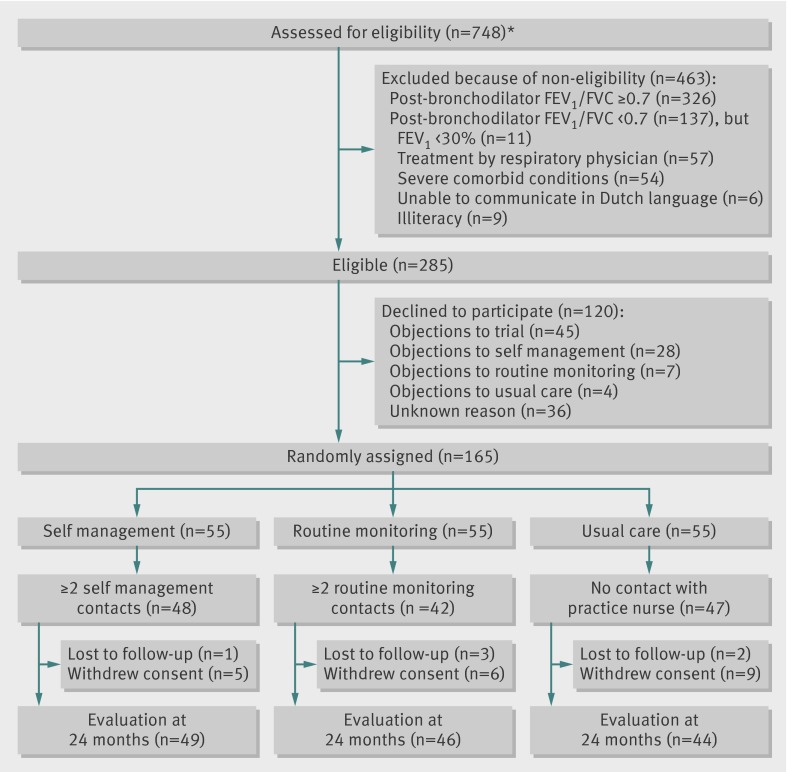
165 patients were allocated to self management (n=55), routine monitoring (n=55), or usual care alone (n=55). At 24 months, adjusted treatment differences between the three groups in mean chronic respiratory questionnaire total score were not significant. Secondary outcomes did not differ, except for exacerbation management. Compared with usual care, more exacerbations in the self management group were managed with bronchodilators (odds ratio 2.81, 95% confidence interval 1.16 to 6.82) and with prednisolone, antibiotics, or both (3.98, 1.10 to 15.58).
Comprehensive self management or routine monitoring did not show long term benefits in terms of quality of life or self efficacy over usual care alone in COPD patients in general practice. Patients in the self management group seemed to be more capable of appropriately managing exacerbations than did those in the usual care group.
Clinical trials NCT00128765.
评估两种不同疾病管理模式(综合自我管理和常规监测)对慢性阻塞性肺疾病(COPD)患者生活质量(主要目标)、加重频率和患者管理以及自我效能(次要目标)的长期影响,在一般实践中。
24 个月,多中心,研究者盲法,三臂,实用,随机对照试验。
荷兰东部的 15 家普通诊所。
通过肺活量测定法确诊的 COPD 患者,并在普通诊所接受治疗。排除非常严重的 COPD 患者或接受呼吸科医生治疗的患者。
综合自我管理方案作为常规护理的辅助手段,包括四次与执业护士进行的个性化辅导课程,并通过执业护士进行持续的电话支持;常规监测作为常规护理的辅助手段,包括每年与执业护士进行 2-4 次结构化咨询;或单独进行常规护理(患者主动与全科医生联系)。
165 名患者被分配到自我管理组(n=55)、常规监测组(n=55)或单独常规护理组(n=55)。24 个月时,三组间慢性呼吸道问卷总分的调整治疗差异无统计学意义。次要结果没有差异,除了加重管理。与常规护理相比,自我管理组更多的加重病例通过支气管扩张剂(比值比 2.81,95%置信区间 1.16 至 6.82)和泼尼松龙、抗生素或两者联合治疗(3.98,1.10 至 15.58)。
在一般实践中的 COPD 患者中,综合自我管理或常规监测并未显示出优于单独常规护理的长期生活质量或自我效能优势。自我管理组的患者似乎比常规护理组的患者更有能力适当管理加重病例。
临床试验 NCT00128765。