Discipline of Public Health, The University of Adelaide, Adelaide, Australia.
PLoS One. 2012;7(11):e50155. doi: 10.1371/journal.pone.0050155. Epub 2012 Nov 30.
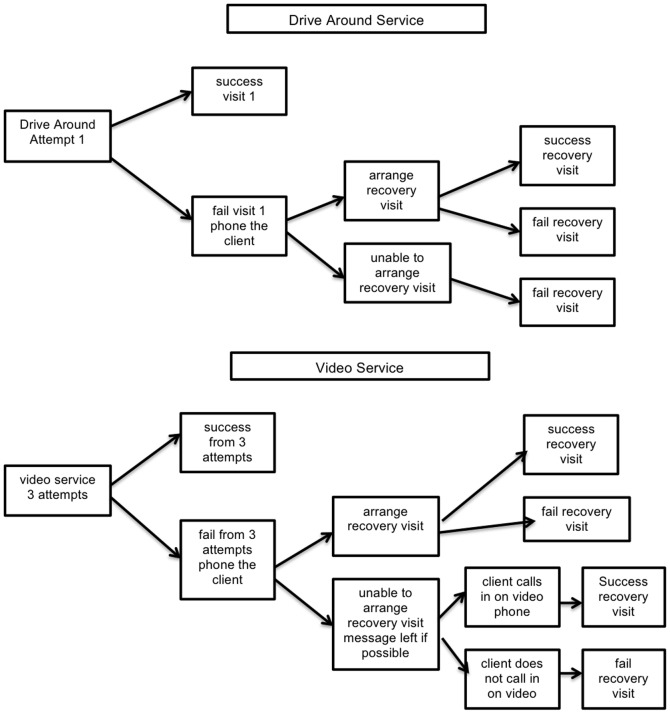
THE USE OF DIRECT OBSERVATION TO MONITOR TUBERCULOSIS TREATMENT IS CONTROVERSIAL: cost, practical difficulties, and lack of patient acceptability limit effectiveness. Telehealth is a promising alternative delivery method for improving implementation. This study aimed to evaluate the clinical and cost-effectiveness of a telehealth service delivering direct observation, compared to an in-person drive-around service.
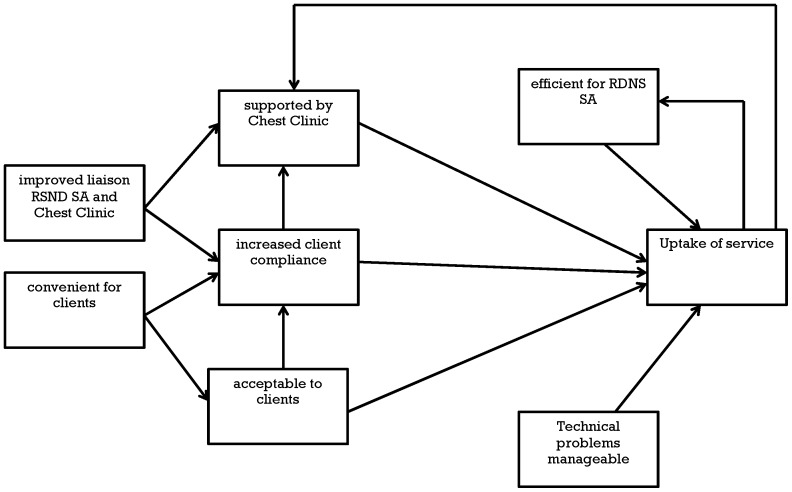
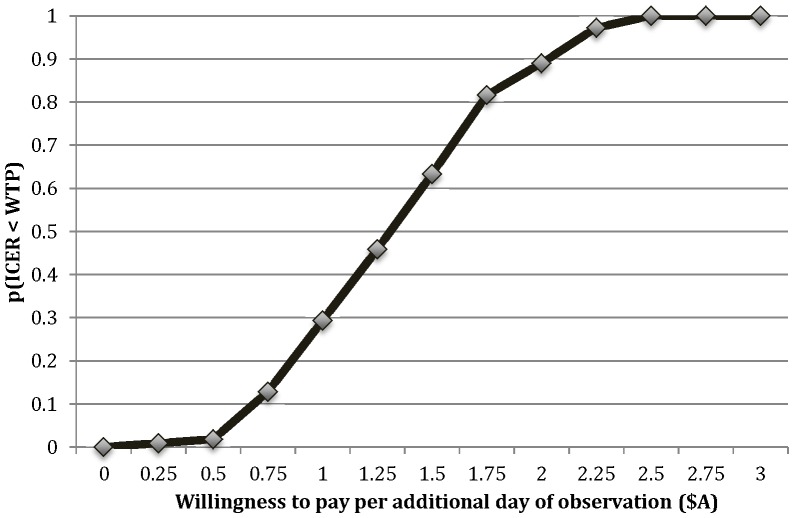
METHODOLOGY/PRINCIPAL FINDINGS: The study was conducted within a community nursing service in South Australia. Telehealth patients received daily video calls at home on a desktop videophone provided by the nursing call center. A retrospective cohort study assessed the effectiveness of the telehealth and traditional forms of observation, defined by the proportion of missed observations recorded in case notes. This data was inputted to a model, estimating the incremental cost-effectiveness ratio (ICER) of telehealth. Semi-structured interviews were conducted with current patients, community nursing and Chest Clinic staff, concerning service acceptability, usability and sustainability. The percentage of missed observations for the telehealth service was 12.1 (n = 58), compared to 31.1 for the in-person service (n = 70). Most of the difference of 18.9% (95% CI: 12.2 - 25.4) was due to fewer pre-arranged absences. The economic analysis calculated the ICER to be AUD$1.32 (95% CI: $0.51 - $2.26) per extra day of successful observation. The video service used less staff time, and became dominant if implemented on a larger scale and/or with decreased technology costs. Qualitative analysis found enabling factors of flexible timing, high patient acceptance, staff efficiency, and Chest Clinic support. Substantial technical problems were manageable, and improved liaison between the nursing service and Chest Clinic was an unexpected side-benefit.
CONCLUSIONS/SIGNIFICANCE: Home video observation is a patient-centered, resource efficient way of delivering direct observation for TB, and is cost-effective when compared with a drive-around service. Future research is recommended to determine applicability and effectiveness in other settings.
直接观察监测结核病治疗存在争议:成本高、实际困难以及患者接受度低限制了其效果。远程医疗是提高实施效果的一种很有前途的替代交付方法。本研究旨在评估远程医疗服务与面对面驱车巡访服务相比在提供直接观察方面的临床和成本效益。
方法/主要发现:该研究在南澳大利亚的社区护理服务中进行。远程医疗患者在家中使用由护理呼叫中心提供的台式可视电话接受每日视频通话。一项回顾性队列研究评估了远程医疗和传统观察形式的有效性,定义为病例记录中记录的漏诊次数比例。该数据输入到模型中,估算了远程医疗的增量成本效益比(ICER)。对当前患者、社区护理和胸科诊所工作人员进行了半结构化访谈,了解服务的可接受性、可用性和可持续性。远程医疗服务的漏诊率为 12.1%(n=58),而面对面服务的漏诊率为 31.1%(n=70)。18.9%的差异(95%CI:12.2-25.4)主要归因于较少的预先安排的缺勤。经济分析计算出的 ICER 为每额外成功观察一天 1.32 澳元(95%CI:0.51-2.26)。视频服务使用的员工时间更少,如果在更大规模实施和/或降低技术成本,则具有优势。定性分析发现了灵活的时间安排、高患者接受度、员工效率和胸科诊所支持等促成因素。重大技术问题是可控的,并且护理服务和胸科诊所之间的联系得到改善是一个意外的好处。
结论/意义:家庭视频观察是一种以患者为中心、资源高效的结核病直接观察方法,与驱车巡访服务相比具有成本效益。建议进行进一步研究,以确定其在其他环境中的适用性和有效性。