Corresponding author: Daniel J. West,
Diabetes Care. 2013 Aug;36(8):2217-24. doi: 10.2337/dc12-2467. Epub 2013 Mar 20.
To examine the acute and 24-h glycemic responses to reductions in postexercise rapid-acting insulin dose in type 1 diabetic patients.
After preliminary testing, 11 male patients (24 ± 2 years, HbA1c 7.7 ± 0.3%; 61 ± 3.4 mmol/mol) attended the laboratory on three mornings. Patients consumed a standardized breakfast (1 g carbohydrate · kg(-1) BM; 380 ± 10 kcal) and self-administered a 25% rapid-acting insulin dose 60 min prior to performing 45 min of treadmill running at 72.5 ± 0.9% VO2peak. At 60 min postexercise, patients ingested a meal (1 g carbohydrate · kg(-1) BM; 660 ± 21 kcal) and administered a Full, 75%, or 50% rapid-acting insulin dose. Blood glucose concentrations were measured for 3 h postmeal. Interstitial glucose was recorded for 20 h after leaving the laboratory using a continuous glucose monitoring system.
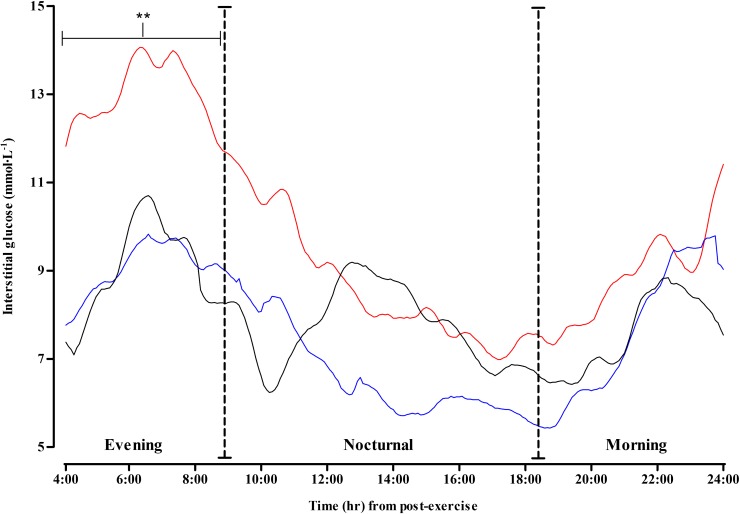
All glycemic responses were similar across conditions up to 60 min postexercise. After the postexercise meal, blood glucose was preserved under 50%, but declined under Full and 75%. Thence at 3 h, blood glucose was highest under 50% (50% [10.4 ± 1.2] vs. Full [6.2 ± 0.7] and 75% [7.6 ± 1.2 mmol · L(-1)], P = 0.029); throughout this period, all patients were protected against hypoglycemia under 50% (blood glucose ≤ 3.9; Full, n = 5; 75%, n = 2; 50%, n = 0). Fifty percent continued to protect patients against hypoglycemia for a further 4 h under free-living conditions. However, late-evening and nocturnal glycemia were similar; as a consequence, late-onset hypoglycemia was experienced under all conditions.
A 25% pre-exercise and 50% postexercise rapid-acting insulin dose preserves glycemia and protects patients against early-onset hypoglycemia (≤ 8 h). However, this strategy does not protect against late-onset postexercise hypoglycemia.
研究在 1 型糖尿病患者中,减少运动后速效胰岛素剂量对急性和 24 小时血糖的影响。
经过初步测试,11 名男性患者(24 ± 2 岁,HbA1c 7.7 ± 0.3%;61 ± 3.4mmol/mol)在三个早上到实验室就诊。患者在进行 45 分钟的跑步机跑步前 60 分钟,摄入一份标准化早餐(1g 碳水化合物·kg(-1) BM;380 ± 10kcal)并自行注射 25%的速效胰岛素剂量。在运动后 60 分钟,患者摄入一份餐食(1g 碳水化合物·kg(-1) BM;660 ± 21kcal)并给予全剂量、75%剂量或 50%剂量的速效胰岛素。在进餐后 3 小时测量血糖浓度。使用连续血糖监测系统在离开实验室后 20 小时记录间质葡萄糖。
在运动后 60 分钟内,所有血糖反应在各条件下均相似。在运动后的餐食后,血糖在 50%的剂量下得到维持,但在全剂量和 75%的剂量下下降。因此,在 3 小时时,血糖在 50%的剂量下最高(50%[10.4 ± 1.2]vs.全剂量[6.2 ± 0.7]和 75%[7.6 ± 1.2mmol·L(-1)],P=0.029);在此期间,所有患者在 50%的剂量下都免受低血糖的影响(血糖≤3.9mmol/L;全剂量,n=5;75%,n=2;50%,n=0)。在自由生活条件下,50%的剂量还能在另外 4 小时内继续保护患者免受低血糖的影响。然而,夜间和深夜的血糖水平相似;因此,在所有条件下都发生了迟发性低血糖。
运动前 25%和运动后 50%的速效胰岛素剂量可维持血糖水平,并预防早期(≤8 小时)低血糖发作。然而,这种策略并不能预防运动后迟发性低血糖。