Aubron Cecile, Cheng Allen C, Pilcher David, Leong Tim, Magrin Geoff, Cooper D Jamie, Scheinkestel Carlos, Pellegrino Vince
Crit Care. 2013 Apr 18;17(2):R73. doi: 10.1186/cc12681.
Mortality of patients on extracorporeal membrane oxygenation (ECMO) remains high. The objectives of this study were to assess the factors associated with outcome of patients undergoing ECMO in a large ECMO referral centre and to compare veno-arterial ECMO (VA ECMO) with veno-venous ECMO (VV ECMO).
We reviewed a prospectively obtained ECMO database and patients' medical records between January 2005 and June 2011. Demographic characteristics, illness severity at admission, ECMO indication, organ failure scores before ECMO and the ECMO mode and configuration were recorded. Bleeding, neurological, vascular and infectious complications that occurred on ECMO were also collected. Demographic, illness, ECMO support descriptors and complications associated with hospital mortality were analysed.
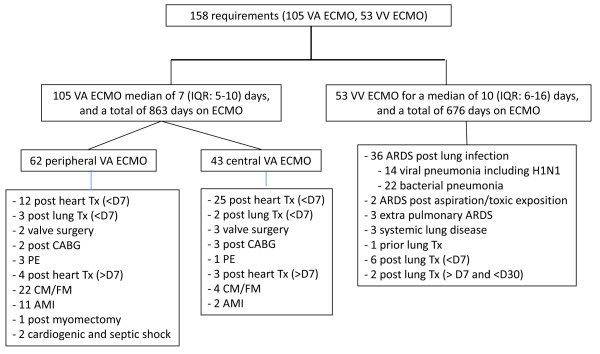
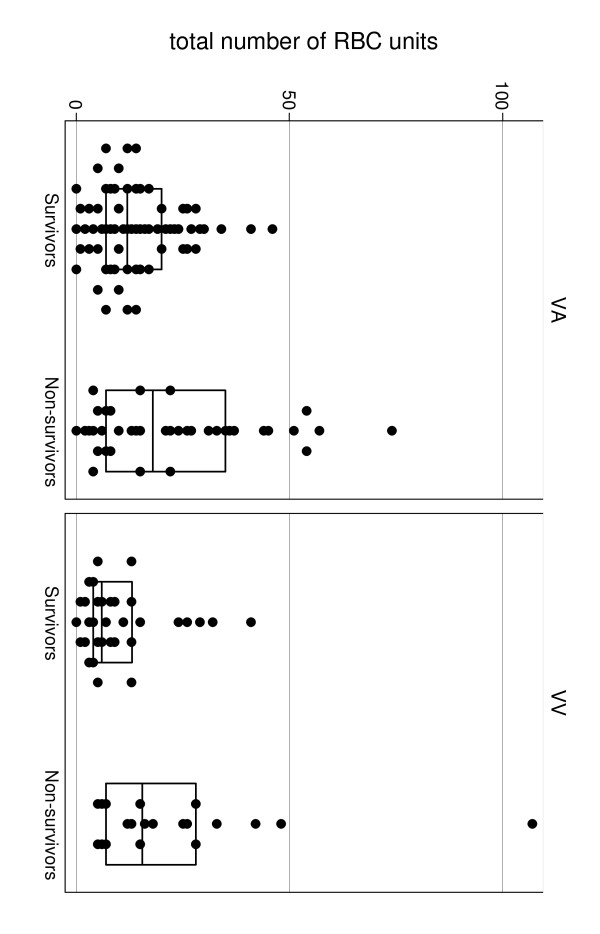
ECMO was initiated 158 times in 151 patients. VA ECMO (66.5%) was twice as common as VV ECMO (33.5%) with a median duration significantly shorter than for VV ECMO (7 days (first and third quartiles: 5; 10 days) versus 10 days (first and third quartiles: 6; 16 days)). The most frequent complications during ECMO support were bleeding and bloodstream infections regardless of ECMO type. More than 70% of the ECMO episodes were successfully weaned in each ECMO group. The overall mortality was 37.3% (37.1% for the patients who underwent VA ECMO, and 37.7% for the patients who underwent VV ECMO). Haemorrhagic events, assessed by the total of red blood cell units received during ECMO, were associated with hospital mortality for both ECMO types.
Among neurologic, vascular, infectious and bleeding events that occurred on ECMO, bleeding was the most frequent and had a significant impact on mortality. Further studies are needed to better investigate bleeding and coagulopathy in these patients. Interventions that reduce these complications may improve outcome.
接受体外膜肺氧合(ECMO)治疗的患者死亡率仍然很高。本研究的目的是评估在一个大型ECMO转诊中心接受ECMO治疗的患者的预后相关因素,并比较静脉-动脉ECMO(VA ECMO)和静脉-静脉ECMO(VV ECMO)。
我们回顾了2005年1月至2011年6月期间前瞻性获取的ECMO数据库和患者病历。记录了人口统计学特征、入院时的疾病严重程度、ECMO适应症、ECMO前的器官衰竭评分以及ECMO模式和配置。还收集了ECMO期间发生的出血、神经、血管和感染并发症。分析了与医院死亡率相关的人口统计学、疾病、ECMO支持描述符和并发症。
151例患者共启动ECMO 158次。VA ECMO(66.5%)的使用频率是VV ECMO(33.5%)的两倍,其持续时间中位数明显短于VV ECMO(7天(第一和第三四分位数:5;10天)对10天(第一和第三四分位数:6;16天))。无论ECMO类型如何,ECMO支持期间最常见的并发症是出血和血流感染。每个ECMO组中超过70%的ECMO治疗过程成功撤机。总体死亡率为37.3%(接受VA ECMO治疗的患者为37.1%,接受VV ECMO治疗的患者为37.7%)。通过ECMO期间接受的红细胞单位总数评估的出血事件与两种ECMO类型的医院死亡率均相关。
在ECMO期间发生的神经、血管、感染和出血事件中,出血最为常见,且对死亡率有显著影响。需要进一步研究以更好地调查这些患者的出血和凝血病。减少这些并发症的干预措施可能会改善预后。