Department of Biopharmaceutical Sciences, College of Pharmacy, University of Illinois at Chicago, 833 S, Wood Street, Chicago, IL 60611, USA.
Mol Cancer. 2013 May 1;12:34. doi: 10.1186/1476-4598-12-34.
Prior to the introduction of tamoxifen, high dose estradiol was used to treat breast cancer patients with similar efficacy as tamoxifen, albeit with some undesirable side effects. There is renewed interest to utilize estradiol to treat endocrine resistant breast cancers, especially since findings from several preclinical models and clinical trials indicate that estradiol may be a rational second-line therapy in patients exhibiting resistance to tamoxifen and/or aromatase inhibitors. We and others reported that breast cancer patients bearing protein kinase C alpha (PKCα)- expressing tumors exhibit endocrine resistance and tumor aggressiveness. Our T47D:A18/PKCα preclinical model is tamoxifen-resistant, hormone-independent, yet is inhibited by 17β-estradiol (E2) in vivo. We previously reported that E2-induced T47D:A18/PKCα tumor regression requires extranuclear ERα and interaction with the extracellular matrix.
T47D:A18/PKCα cells were grown in vitro using two-dimensional (2D) cell culture, three-dimensional (3D) Matrigel and in vivo by establishing xenografts in athymic mice. Immunofluoresence confocal microscopy and co-localization were applied to determine estrogen receptor alpha (ERα) subcellular localization. Co-immunoprecipitation and western blot were used to examine interaction of ERα with caveolin-1.
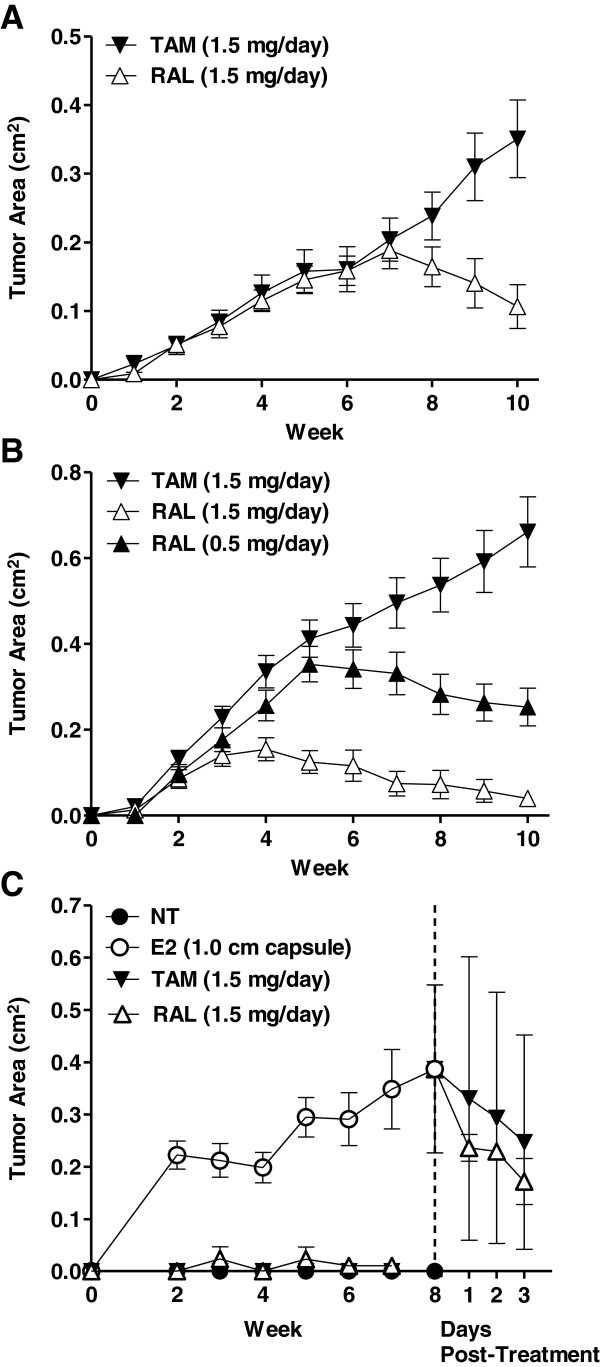
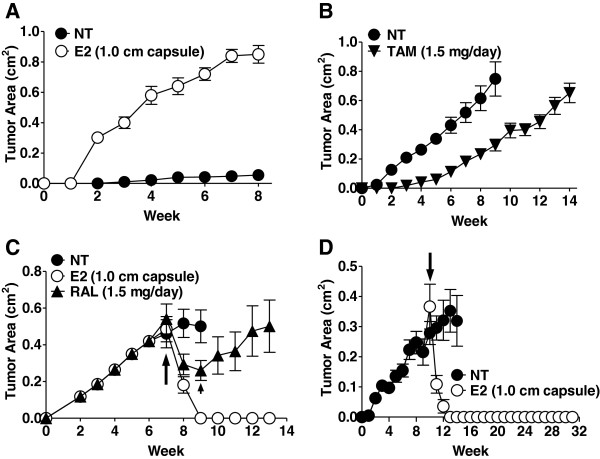
We report that although T47D:A18/PKCα cells are cross-resistant to raloxifene in cell culture and in Matrigel, raloxifene induces regression of tamoxifen-resistant tumors. ERα rapidly translocates to extranuclear sites during T47D:A18/PKCα tumor regression in response to both raloxifene and E2, whereas ERα is primarily localized in the nucleus in proliferating tumors. E2 treatment induced complete tumor regression whereas cessation of raloxifene treatment resulted in tumor regrowth accompanied by re-localization of ERα to the nucleus. T47D:A18/neo tumors that do not overexpress PKCα maintain ERα in the nucleus during tamoxifen-mediated regression. An association between ERα and caveolin-1 increases in tumors regressing in response to E2.
Extranuclear ERα plays a role in the regression of PKCα-overexpressing tamoxifen-resistant tumors. These studies underline the unique role of extranuclear ERα in E2- and raloxifene-induced tumor regression that may have implications for treatment of endocrine-resistant PKCα-expressing tumors encountered in the clinic.
在他莫昔芬问世之前,高剂量雌二醇被用于治疗乳腺癌患者,其疗效与他莫昔芬相似,但存在一些不良副作用。人们对利用雌二醇治疗内分泌抵抗性乳腺癌重新产生了兴趣,特别是因为来自几个临床前模型和临床试验的发现表明,雌二醇可能是对他莫昔芬和/或芳香化酶抑制剂耐药的患者的合理二线治疗。我们和其他人报道称,携带蛋白激酶 C 阿尔法(PKCα)表达肿瘤的乳腺癌患者表现出内分泌抵抗和肿瘤侵袭性。我们的 T47D:A18/PKCα 临床前模型对他莫昔芬耐药,激素独立,但在体内被 17β-雌二醇(E2)抑制。我们之前报道过,E2 诱导的 T47D:A18/PKCα 肿瘤消退需要核外 ERα 并与细胞外基质相互作用。
T47D:A18/PKCα 细胞在体外通过二维(2D)细胞培养、三维(3D)Matrigel 以及在无胸腺小鼠中建立异种移植物进行培养。应用免疫荧光共聚焦显微镜和共定位来确定雌激素受体 alpha(ERα)的亚细胞定位。应用共免疫沉淀和 Western blot 来检测 ERα 与 caveolin-1 的相互作用。
我们报告称,尽管 T47D:A18/PKCα 细胞在细胞培养和 Matrigel 中对雷洛昔芬交叉耐药,但雷洛昔芬可诱导他莫昔芬耐药肿瘤消退。在 T47D:A18/PKCα 肿瘤对雷洛昔芬和 E2 产生反应时,ERα 迅速转位到核外部位,而 ERα 在增殖肿瘤中主要位于核内。E2 治疗诱导完全肿瘤消退,而雷洛昔芬治疗停止导致肿瘤复发,同时 ERα 重新定位到核内。在他莫昔芬介导的消退过程中不过度表达 PKCα 的 T47D:A18/neo 肿瘤保持 ERα 在核内。在对 E2 产生反应时,ERα 与 caveolin-1 的关联增加。
核外 ERα 在 PKCα 过表达的他莫昔芬耐药肿瘤的消退中发挥作用。这些研究强调了核外 ERα 在 E2 和雷洛昔芬诱导的肿瘤消退中的独特作用,这可能对治疗临床上遇到的内分泌抵抗性 PKCα 表达肿瘤具有重要意义。