Faculty of Medicine, Centre for Health Systems and Safety Research, Australian Institute of Health Innovation, University of New South Wales, Sydney, New South Wales, Australia.
J Am Med Inform Assoc. 2013 Nov-Dec;20(6):1159-67. doi: 10.1136/amiajnl-2013-001745. Epub 2013 May 30.
To compare the manifestations, mechanisms, and rates of system-related errors associated with two electronic prescribing systems (e-PS). To determine if the rate of system-related prescribing errors is greater than the rate of errors prevented.
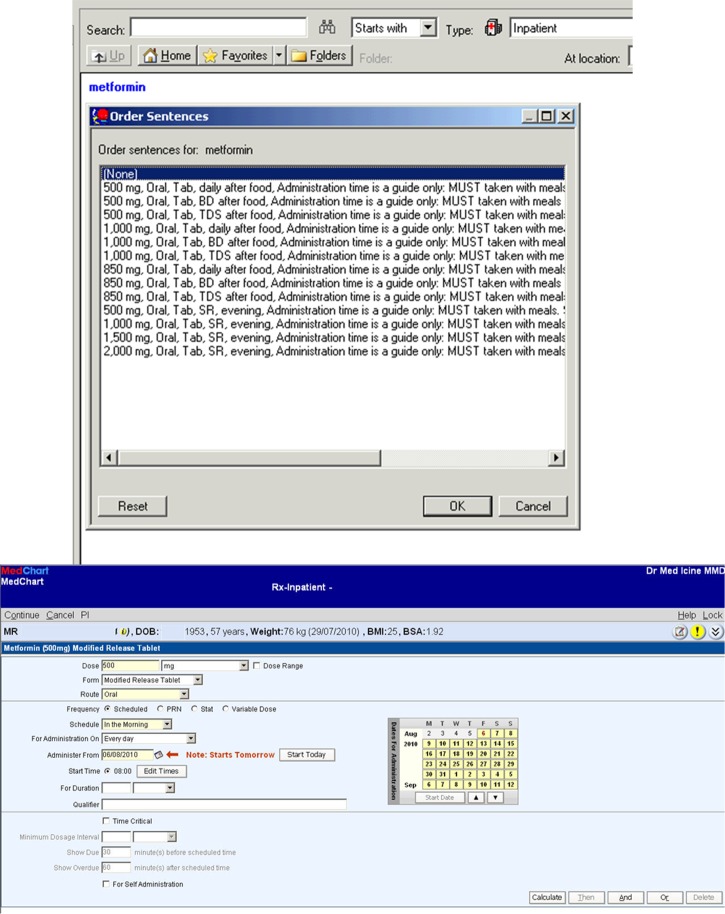
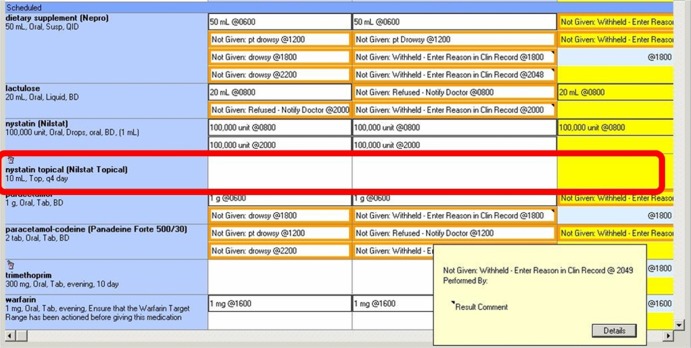
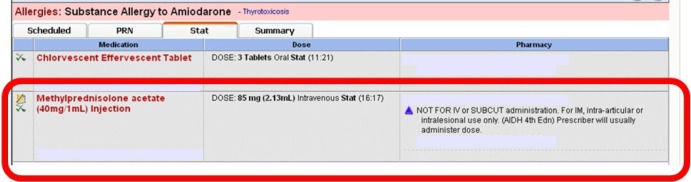
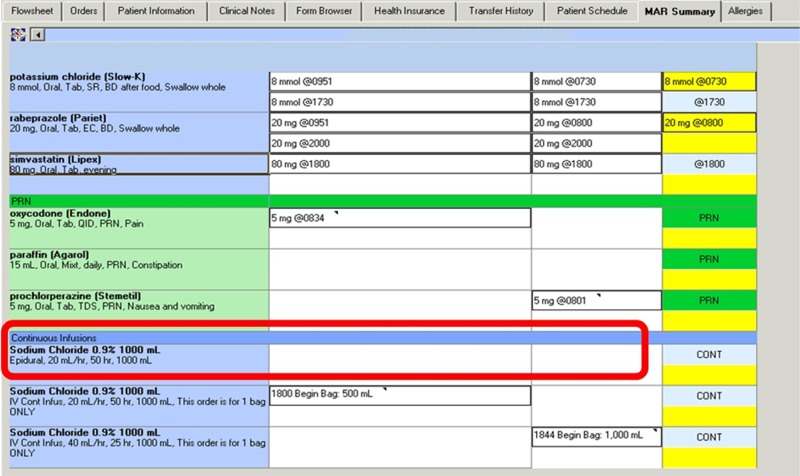
Audit of 629 inpatient admissions at two hospitals in Sydney, Australia using the CSC MedChart and Cerner Millennium e-PS. System related errors were classified by manifestation (eg, wrong dose), mechanism, and severity. A mechanism typology comprised errors made: selecting items from drop-down menus; constructing orders; editing orders; or failing to complete new e-PS tasks. Proportions and rates of errors by manifestation, mechanism, and e-PS were calculated.
42.4% (n=493) of 1164 prescribing errors were system-related (78/100 admissions). This result did not differ by e-PS (MedChart 42.6% (95% CI 39.1 to 46.1); Cerner 41.9% (37.1 to 46.8)). For 13.4% (n=66) of system-related errors there was evidence that the error was detected prior to study audit. 27.4% (n=135) of system-related errors manifested as timing errors and 22.5% (n=111) wrong drug strength errors. Selection errors accounted for 43.4% (34.2/100 admissions), editing errors 21.1% (16.5/100 admissions), and failure to complete new e-PS tasks 32.0% (32.0/100 admissions). MedChart generated more selection errors (OR=4.17; p=0.00002) but fewer new task failures (OR=0.37; p=0.003) relative to the Cerner e-PS. The two systems prevented significantly more errors than they generated (220/100 admissions (95% CI 180 to 261) vs 78 (95% CI 66 to 91)).
System-related errors are frequent, yet few are detected. e-PS require new tasks of prescribers, creating additional cognitive load and error opportunities. Dual classification, by manifestation and mechanism, allowed identification of design features which increase risk and potential solutions. e-PS designs with fewer drop-down menu selections may reduce error risk.
比较两种电子医嘱系统(e-PS)相关的表现、机制和系统相关错误率。确定系统相关的处方错误率是否大于预防的错误率。
对澳大利亚悉尼两家医院的 629 例住院患者进行审核,使用 CSC MedChart 和 Cerner Millennium e-PS。系统相关错误按表现(例如,剂量错误)、机制和严重程度进行分类。机制分类包括从下拉菜单中选择项目、构建医嘱、编辑医嘱或未能完成新的 e-PS 任务。按表现、机制和 e-PS 计算错误的比例和发生率。
1164 个处方错误中有 42.4%(493/1164)为系统相关(78/100 个入院)。这一结果在两种 e-PS 之间没有差异(MedChart 为 42.6%(95%CI 39.1 至 46.1);Cerner 为 41.9%(37.1 至 46.8))。对于 13.4%(66/500)的系统相关错误,有证据表明该错误在研究审核之前就已经被发现。27.4%(135/500)的系统相关错误表现为时间错误,22.5%(111/500)为药物强度错误。选择错误占 43.4%(34.2/100 个入院),编辑错误占 21.1%(16.5/100 个入院),未能完成新的 e-PS 任务占 32.0%(32.0/100 个入院)。MedChart 生成的选择错误(OR=4.17;p=0.00002)更多,但生成的新任务失败(OR=0.37;p=0.003)更少。与 Cerner e-PS 相比,这两种系统预防的错误明显多于生成的错误(220/100 个入院(95%CI 180 至 261)与 78(95%CI 66 至 91))。
系统相关错误很常见,但很少被发现。电子医嘱系统需要医生执行新任务,这增加了认知负荷和错误机会。通过表现和机制进行双重分类,可以确定增加风险和潜在解决方案的设计特征。减少下拉菜单选择数量的电子医嘱系统设计可能会降低错误风险。