Department of Molecular Medicine and Surgery, Karolinska Institutet and Center for Surgical Gastroenterology, Karolinska University Hospital, Solna P9:03, SE 171 76 Stockholm, Sweden.
BMC Cancer. 2013 Jun 7;13:279. doi: 10.1186/1471-2407-13-279.
Current standard for most of the locally advanced rectal cancers is preoperative chemoradiotherapy, and, variably per institution, postoperative adjuvant chemotherapy. Short-course preoperative radiation with delayed surgery has been shown to induce tumour down-staging in both randomized and observational studies. The concept of neo-adjuvant chemotherapy has been proven successful in gastric cancer, hepatic metastases from colorectal cancer and is currently tested in primary colon cancer.
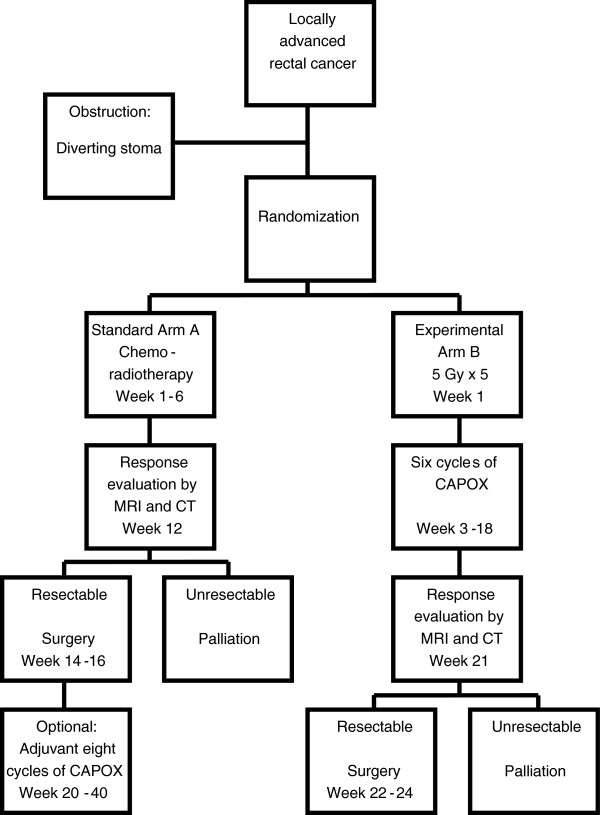
Patients with rectal cancer with high risk features for local or systemic failure on magnetic resonance imaging are randomized to either a standard arm or an experimental arm. The standard arm consists of chemoradiation (1.8 Gy x 25 or 2 Gy x 25 with capecitabine) preoperatively, followed by selective postoperative adjuvant chemotherapy. Postoperative chemotherapy is optional and may be omitted by participating institutions. The experimental arm includes short-course radiotherapy (5 Gy x 5) followed by full-dose chemotherapy (capecitabine and oxaliplatin) in 6 cycles before surgery. In the experimental arm, no postoperative chemotherapy is prescribed. Surgery is performed according to TME principles in both study arms. The hypothesis is that short-course radiotherapy with neo-adjuvant chemotherapy increases disease-free and overall survival without compromising local control. Primary end-point is disease-free survival at 3 years. Secondary endpoints include overall survival, local control, toxicity profile, and treatment completion rate, rate of pathological complete response and microscopically radical resection, and quality of life.
Following the advances in rectal cancer management, increased focus on survival rather than only on local control is now justified. In an experimental arm, short-course radiotherapy is combined with full-dose chemotherapy preoperatively, an alternative that offers advantages compared to concomitant chemoradiotherapy with or without postoperative chemotherapy. In a multi-centre setting this regimen is compared to current standard with the aim of improving survival for patients with locally advanced rectal cancer.
ClinicalTrials.gov NCT01558921.
目前,大多数局部进展期直肠癌的标准治疗方案是术前放化疗,以及根据不同机构的情况,术后辅助化疗。短程术前放疗加延迟手术已在随机和观察性研究中显示出诱导肿瘤降期的作用。新辅助化疗的概念已在胃癌、结直肠癌肝转移中得到证实,并正在原发性结肠癌中进行测试。
对磁共振成像显示局部或全身复发高风险特征的直肠癌患者进行随机分组,分为标准组或实验组。标准组包括术前放化疗(1.8 Gy x 25 或 2 Gy x 25,并用卡培他滨),然后选择性进行术后辅助化疗。术后化疗是可选的,参与机构可能会选择不进行。实验组包括短程放疗(5 Gy x 5),然后在手术前进行 6 个周期的全剂量化疗(卡培他滨和奥沙利铂)。实验组不规定术后化疗。两组研究均按照 TME 原则进行手术。假设短程放疗联合新辅助化疗可提高无病生存率和总生存率,而不会影响局部控制。主要终点是 3 年无病生存率。次要终点包括总生存率、局部控制率、毒性谱、治疗完成率、病理完全缓解率和显微镜下根治性切除率以及生活质量。
随着直肠癌治疗的进展,现在有理由更加关注生存而不仅仅是局部控制。在实验组中,短程放疗与术前全剂量化疗相结合,与同期放化疗加或不加术后化疗相比,提供了优势。在多中心环境中,这种方案与当前的标准方案进行比较,旨在为局部进展期直肠癌患者提高生存率。
ClinicalTrials.gov NCT01558921。